The primary goal of a Cardio-Pulmonary Exercise Test (CPET) is to determine an individual’s maximum oxygen consumption (VO2), minute ventilation (Ve) and heart rate (HR). An adequate CPET is usually indicated by a Respiratory Quotient (VCO2/VO2) that is greater than 1.10, a heart rate greater than 85% of predicted or a Ve greater than 85% of predicted. There are a variety of reasons why patients are unable to exercise to their maximum. Although these reasons can of course include poor motivation, factors such a musculo-skeletal limitations or concerns about patient safety due to EKG changes can cause patients have a sub-maximal test.
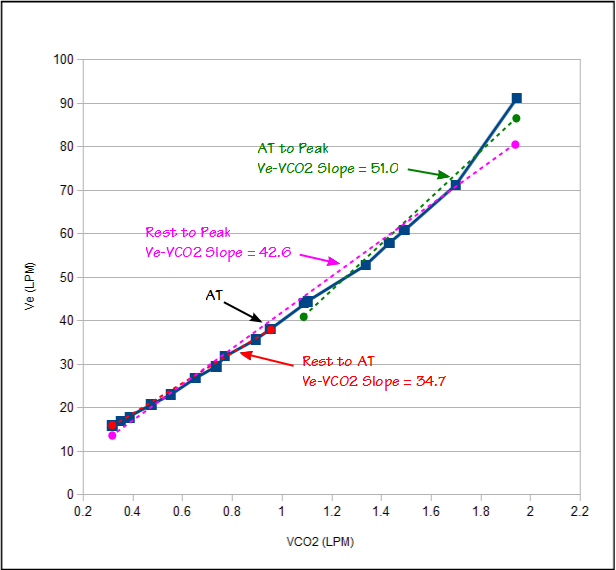
Assessing a sub-maximal test is problematic but there are a number of derived CPET values that have been shown to be useful indicators even when the amount of test data is limited. We have used the Ve-VCO2 slope as one of these indicators for quite a while. Ve-VCO2 slope can be calculated using the Ve and VCO2 from the entire CPET or from just the pre-anaerobic threshold data. Given that there is usually a different Ve-VCO2 slope after AT that is influenced by lactic acidosis as well as VCO2 compared to the slope before AT our preference has been to use only pre-AT data. This means that a CPET can be significantly sub-maximal and we can still get an accurate Ve-VCO2 slope.
The Ve-VCO2 slope is primarily sensitive to the match between ventilation and perfusion in the lung. There is a loose correlation between the Ve-VCO2 slope and cardiac disease and this is usually because of the pulmonary consequences of cardiac disease, not because it is necessarily sensitive to cardiac output or peripheral vascular disease.
An individual’s maximum VO2 is a significant indicator of morbidity and mortality from cardiac disease but when a CPET is sub-maximal the VO2 will be as well. The Ve-VCO2 slope does not correlate well with maximum VO2 and cannot be used as a way to estimate it. A number of investigators however, have shown that the Oxygen Uptake Efficiency Slope (OUES) strongly correlates with maximum VO2 and that OUES can be calculated from sub-maximal CPET test data.
Continue reading →