As workload increases during a progressive cardiopulmonary exercise test (CPET) there comes a point at which the amount of oxygen delivered to the exercising muscle is no longer able to meet its needs. This is the point at which lactic acid begins to accumulate, CO2 production increases and is the accepted definition of the Anaerobic Threshold (AT). The “gold” standard for determining AT is lactic acid measurements but these require sampling blood at regular intervals throughout the CPET. AT is far more commonly determined from respiratory parameters.
Recently I had the opportunity to observe a CPET performed at another PFT Lab. Following the CPET I saw that there was some difficulty in determining the AT. Part of the reason for this is that the staff had only been shown the V-slope method and weren’t aware that there are several alternative approaches.
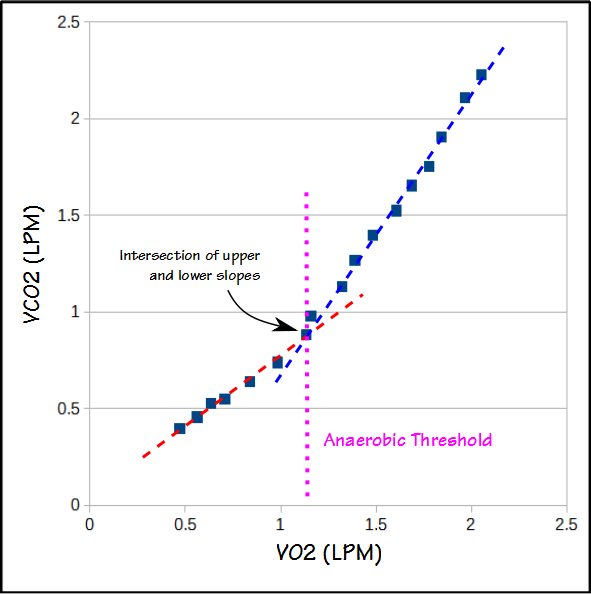
The V-slope method graphs VCO2 versus VO2. The slope of relationship between VCO2 and VO2 both above and below AT is relatively linear, but changes at AT.