Over the last couple of weeks I’ve had an unusual number of patients with expiratory plateaus on their flow-volume loops. Expiratory plateaus are usually considered to be a sign of an intrathoracic central or upper airway obstruction and several of these patients had a diagnosis of tracheomalacia but many of them didn’t. Expiratory (and inspiratory) plateaus are mentioned in the ATS/ERS standards for interpretation but since there isn’t a specific definition (other than “plateau”), an expiratory plateau is a “know it when you see it” sort of thing.
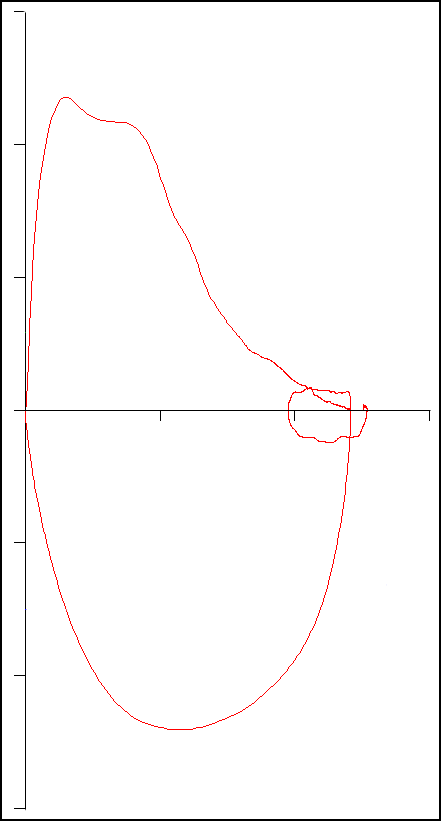
The word plateau tends to imply that the flow-volume loop is both flat and level. Most textbook examples of an expiratory plateau tend to show a flow-volume loop that has been perfectly truncated, usually something like this:

or this:
but it usually isn’t that simple. An expiratory plateau is a consequence of a flow limitation, but during a forced exhalation the diameter of the airways decreases as the lung volume decreases from TLC towards RV. Depending on what is causing the flow limitation the plateau isn’t necessarily flat or level.
So it’s necessary to be a bit flexible when assessing a flow-volume loop for the presence of an expiratory plateau. But given the variability seen in routine spirometry, it’s possible for a subject to produce a single flow-volume loop that looks like it has an expiratory plateau and yet have this feature missing from their remaining spirometry efforts. For this reason the ATS/ERS statement on interpretation also states:
“at least three maximal and repeatable … expiratory flow curves are necessary..”
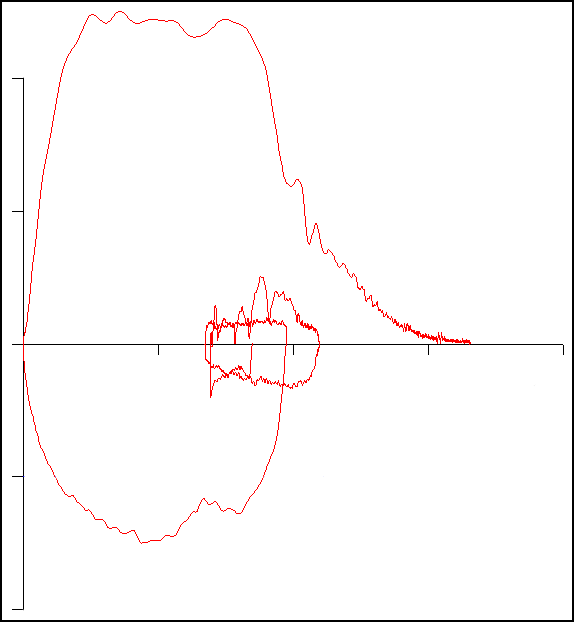
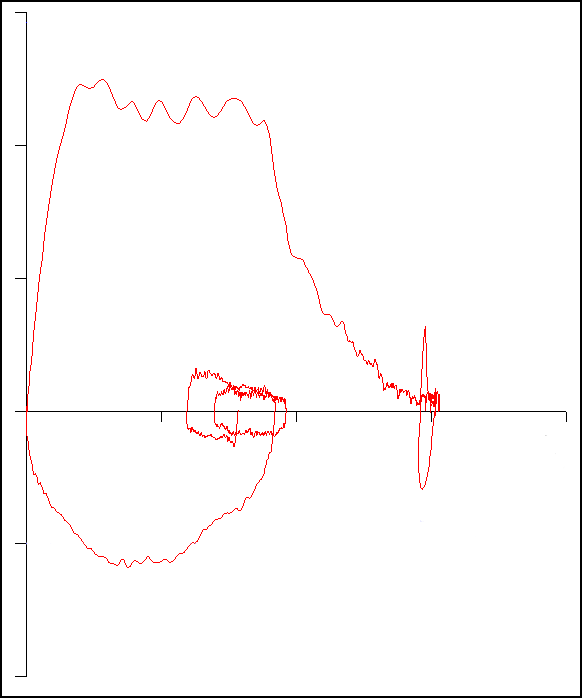
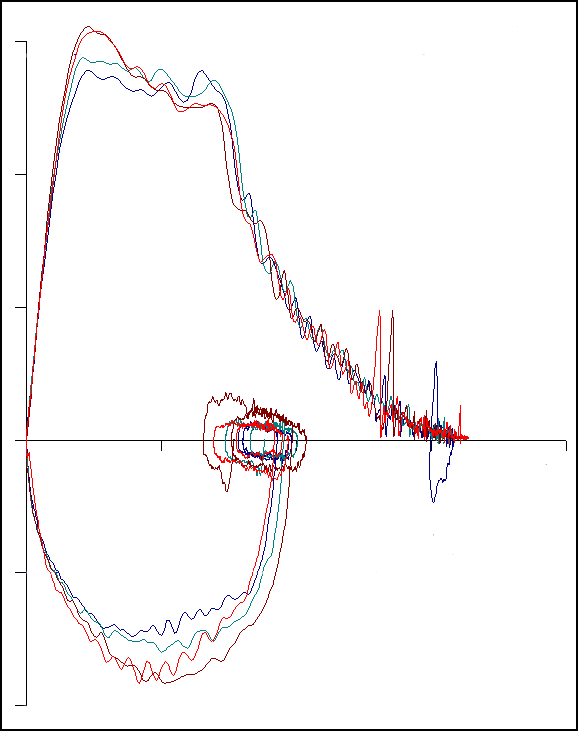
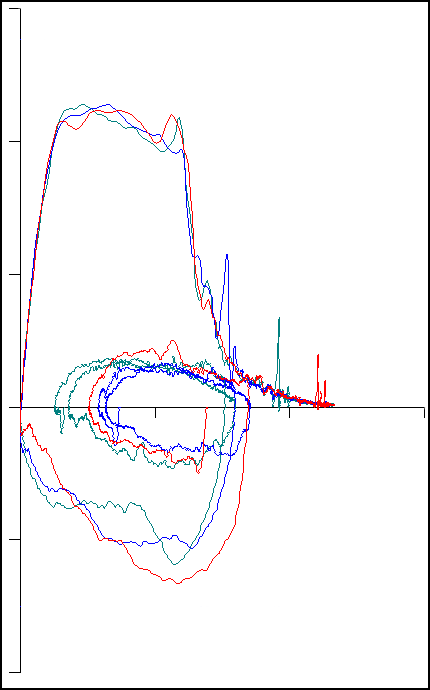
but this also leaves the definition of repeatability in the air. Repeatability is therefore also a “know it when you see it” sort of thing. These spirometry tests show good reapeatability:
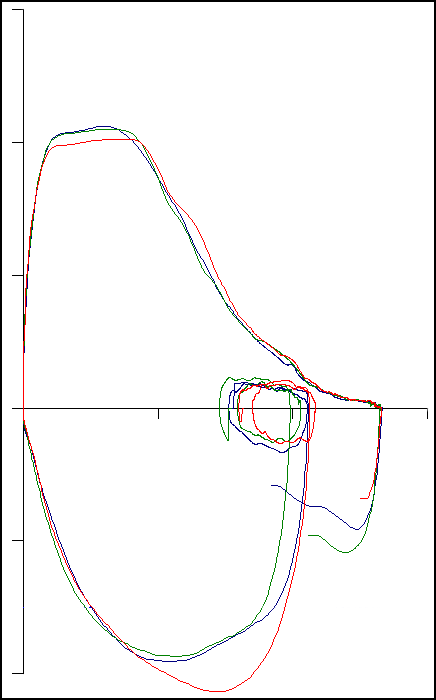
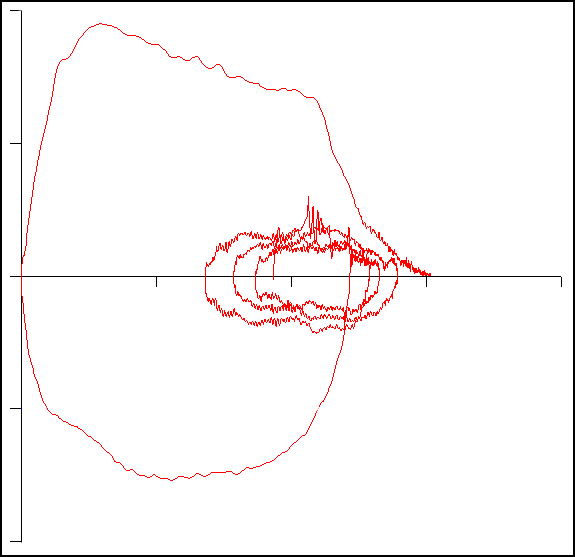
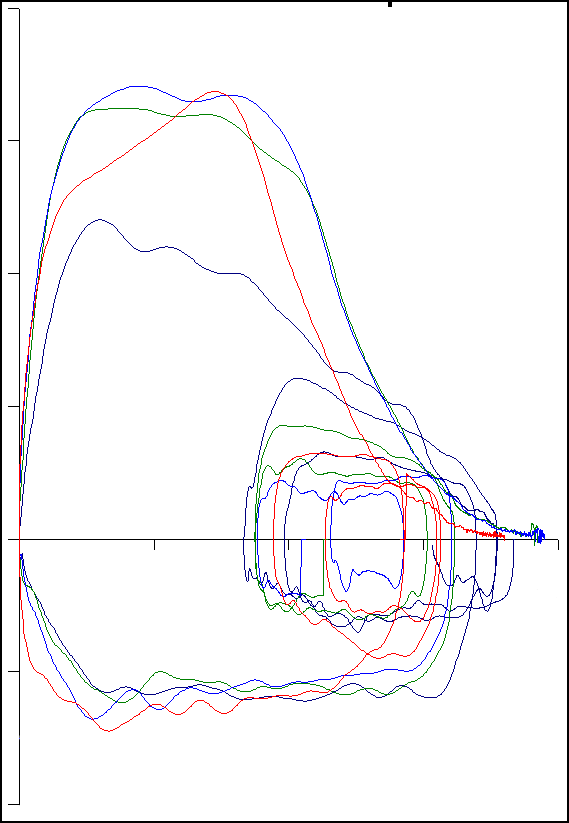
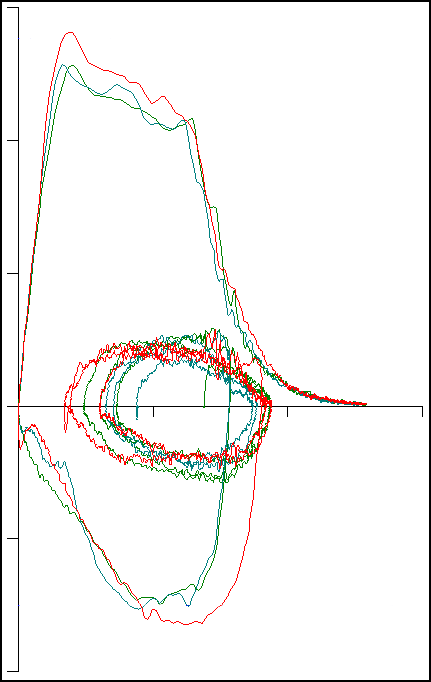
So there’s probably no question that these subjects have an expiratory plateau. These spirometry tests on the other hand show only fair repeatability:
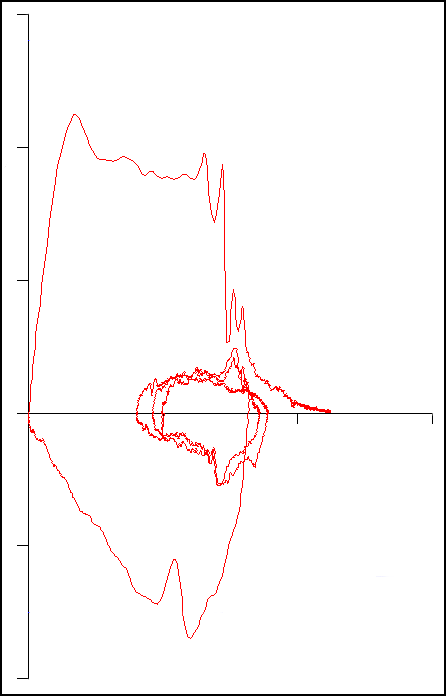
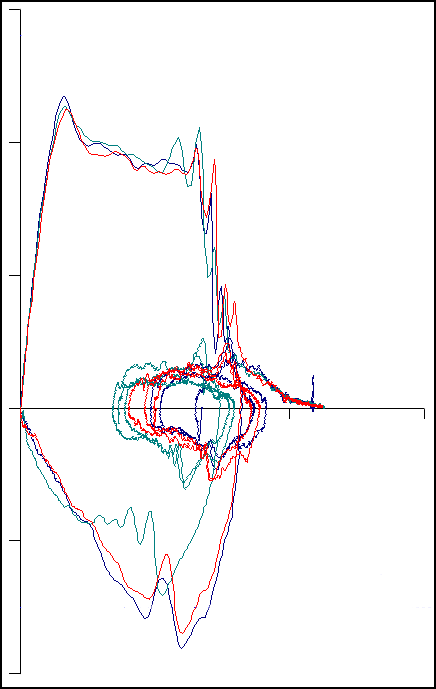
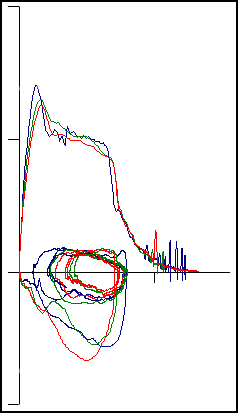
For these subjects it’s not as clear their expiratory plateau is “real”, but they’re probably repeatable enough to be acceptable. These spirometry tests however, show poor repeatability:
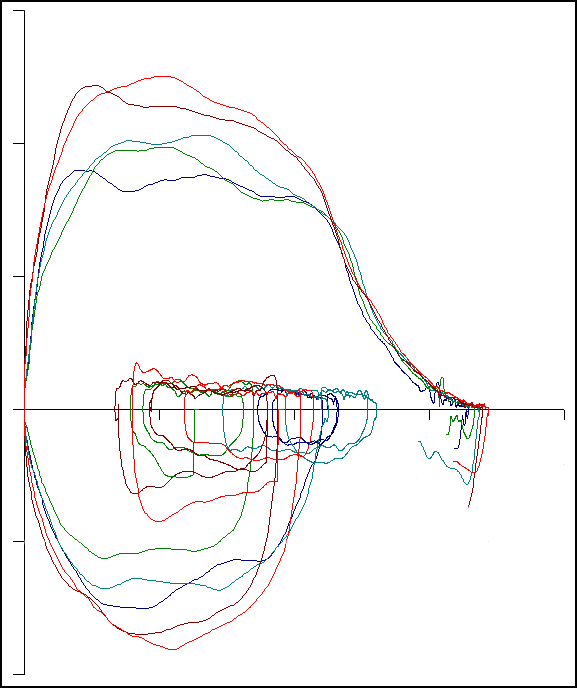
and the variability of these flow-volume loops is large enough that any apparent expiratory plateau is more likely due to poor effort than to an actual expiratory flow limitation.
One interesting question is how repeatable are expiratory plateaus over time? This probably depends on what the underlying cause is. Since close to half the patients we see with an expiratory plateau have a diagnosis of tracheomalacia and are seen in the Airway Clinic that’s run by the hospital’s CardioThoracic Division. The clinic’s surgeons implant airway stents and do tracheal re-constructions so the contour of these patients’ flow-volume loops often changes dramatically from one visit to another.
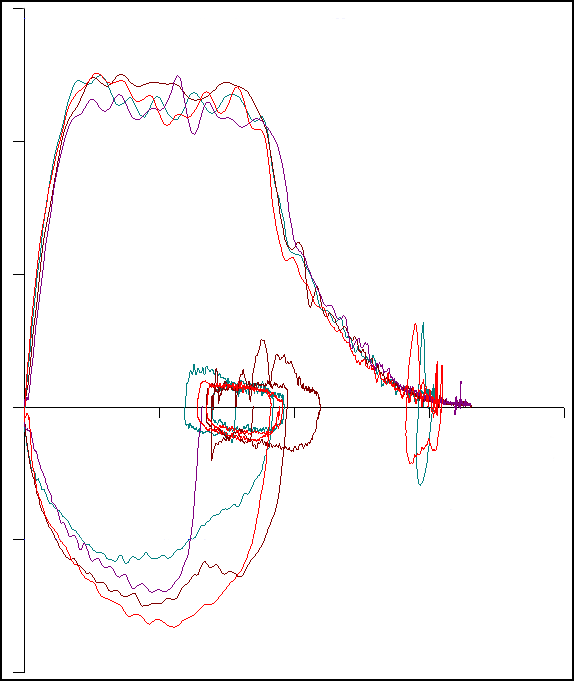
While searching our records for trends in expiratory plateaus however, I found an interesting progression:
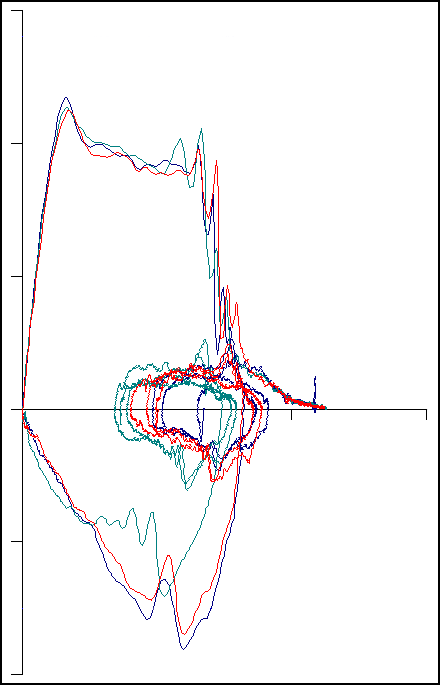
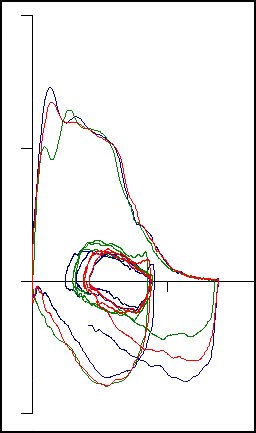
These flow-volume loops come from a patient with a diagnosis of SOB and were performed at approximately roughly6-month intervals over a period of about 2 years. The FEV1, FVC and FEV1/FVC ratios were always within normal limits and did not change significantly from visit to visit but the contour progresses from one that has a very clear expiratory plateau to one that would be considered to be normal. The “shoulder” in the final series of flow-volume loops is even similar to the flow-volume loop labeled as normal in the ATS/ERS standards for spirometry:
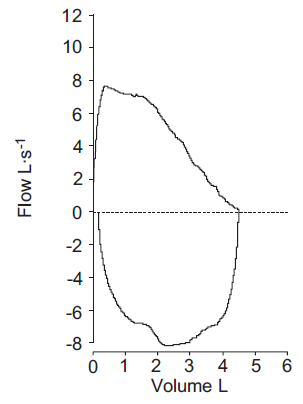
This could of course just be the resolution of whatever was causing the expiratory flow limitation over time (which was never explicitly diagnosed), but it has been suggested that a “shoulder” on a flow-volume loop, even though it is “normal”, may actually a sign of flow limitation. What this makes me wonder is whether some individuals that have a “shoulder” on their flow-volume loop would at one time or another also show an expiratory plateau.
The presence of an expiratory plateau is to some extent in the eye of the beholder. Despite some staff education on my part when I see an expiratory plateau mentioned in the technician notes at all it’s usually that they were “blunted peak flows”. From my point of view a “blunted peak flow” is a low, rounded flow-volume loop with no sign of flattening. This is usually an indication of an inadequate patient effort and I don’t think this looks a lot like an expiratory plateau at all.
This probably means I need to improve the staff education about expiratory plateaus but despite seeing so many expiratory plateaus recently and despite the fact that we see a number of patients from the Airway Clinic that have them they usually aren’t that common. There’s also the fact that good expiratory plateau reproducibility is actually somewhat rare. Fair reproducibility (at best) is a lot more common so to some extent I can understand their confusion.
Expiratory plateaus are a sign of an intrathoracic central or upper airway obstruction. The causes of this kind of obstruction are varied and range from tracheomalacia to goiter and airway tumors. An expiratory plateau is not specific to any one of these conditions however, and does not accurately predict the site or extent of the obstruction. For this reason the ATS/ERS standards for interpretation states:
“…endoscopic and radiological techniques are the next step to confirm this dysfunction.”
Since the FVC and FEV1 often remain normal until the plateau and peak flow are moderately reduced, this form of airway obstruction that can usually only be diagnosed from the contour of the flow-volume loop. For this reason an expiratory plateau should never be ignored but at the same time it needs to be repeatable in order to be sure it isn’t just a fluke.
References:
Brusasco V, Crapo R, Viegi G. ATS/ERS Task Force: Standardisation of lung function testing. Standardisation of spirometry. Eur Respir J 2005; 26: 319-338.
Brusasco V, Crapo R, Viegi G. ATS/ERS Task Force: Standardisation of lung function testing. Interpretive strategies for lung function tests. Eur Respir J 2005; 26: 948-969.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
What is SOB?
Andrey –
Shortness of Breath. Dyspnea.
Regards, Richard
Thank.