The primary goal of a Cardio-Pulmonary Exercise Test (CPET) is to determine an individual’s maximum oxygen consumption (VO2), minute ventilation (Ve) and heart rate (HR). An adequate CPET is usually indicated by a Respiratory Quotient (VCO2/VO2) that is greater than 1.10, a heart rate greater than 85% of predicted or a Ve greater than 85% of predicted. There are a variety of reasons why patients are unable to exercise to their maximum. Although these reasons can of course include poor motivation, factors such a musculo-skeletal limitations or concerns about patient safety due to EKG changes can cause patients have a sub-maximal test.
Assessing a sub-maximal test is problematic but there are a number of derived CPET values that have been shown to be useful indicators even when the amount of test data is limited. We have used the Ve-VCO2 slope as one of these indicators for quite a while. Ve-VCO2 slope can be calculated using the Ve and VCO2 from the entire CPET or from just the pre-anaerobic threshold data. Given that there is usually a different Ve-VCO2 slope after AT that is influenced by lactic acidosis as well as VCO2 compared to the slope before AT our preference has been to use only pre-AT data. This means that a CPET can be significantly sub-maximal and we can still get an accurate Ve-VCO2 slope.
The Ve-VCO2 slope is primarily sensitive to the match between ventilation and perfusion in the lung. There is a loose correlation between the Ve-VCO2 slope and cardiac disease and this is usually because of the pulmonary consequences of cardiac disease, not because it is necessarily sensitive to cardiac output or peripheral vascular disease.
An individual’s maximum VO2 is a significant indicator of morbidity and mortality from cardiac disease but when a CPET is sub-maximal the VO2 will be as well. The Ve-VCO2 slope does not correlate well with maximum VO2 and cannot be used as a way to estimate it. A number of investigators however, have shown that the Oxygen Uptake Efficiency Slope (OUES) strongly correlates with maximum VO2 and that OUES can be calculated from sub-maximal CPET test data.
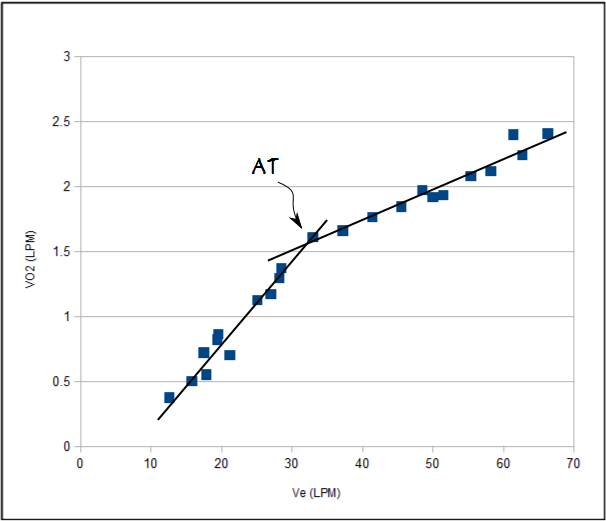
OUES is a function of VO2 and Ve. Ve/VO2 has been on CPET reports for almost as long as I have been doing exercise tests but I have had difficulty seeing its value. The primary reason for this is that an individual’s ventilation during exercise is driven by PaCO2 and acidosis, not PaO2. Like the Ve-VCO2 slope, the Ve-VO2 slope is relatively linear up to anaerobic threshold but after AT, it diverges strongly and can even become alinear.
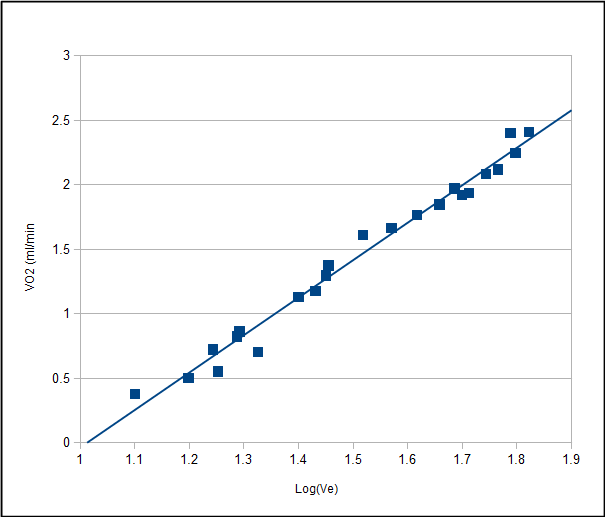
It is for this reason the OUES is derived from the slope of VO2 versus Log Ve and this slope is actually reasonably linear over the course of an entire exercise test.
 A steeper slope and a higher OUES represents a more efficient oxygen uptake while a lower OUES shows that a higher amount of ventilation is required for a given oxygen uptake. Like the maximum VO2 OUES increases with increasing height and decreases with increasing age.
A steeper slope and a higher OUES represents a more efficient oxygen uptake while a lower OUES shows that a higher amount of ventilation is required for a given oxygen uptake. Like the maximum VO2 OUES increases with increasing height and decreases with increasing age.
OUES has been studied using 50%, 75%, 90% and 100% of the data from a CPET study and has been shown to produce similar results and to show an excellent correlation with the maximum VO2 across this range. For this reason it has the ability to act as a surrogate value for VO2 during a sub-maximal test.
OUES is sometimes reported using VO2 as ml/min and sometimes with VO2 as Liters/min. A few investigators have used weight corrected VO2 (i.e. ml/kg/min) but is unclear that this has added any precision to the calculations or analysis of the results.
Reference equations from Hollenberg et al, published in 2000, indicates that for males OUES (in ml/min/log(L/min)) is:
1320 – (26.7 x age) + (1.394 x BSA)
and for females:
1175 – (15.8 x age) + (841 x BSA)
A more recent set of reference equations from Sun et al, published in 2012 indicates that (in L/min/log(L/min)) OUES for males is:
-1.178 – (age x 0.032) + (0.023 x height (cm)) + (0.008 x weight (kg))
and for females it is:
-0.61 – (age x 0.032) + (0.023 x height (cm)) + (0.008 x weight (kg))
OUES has been studied almost exclusively in normal subjects and those with cardiac disease. Since the correlation between OUES and maximum VO2 depends on a normal arterial-venous oxygen gradient it is not clear how effective OUES is as a prognostic factor in patients with pulmonary disease. The relationship between OUES and maximum VO2 has been studied however, in subjects breathing a hypoxic gas mixture and in patients with pulmonary hypertension, and the correlation remained very good in both instances.
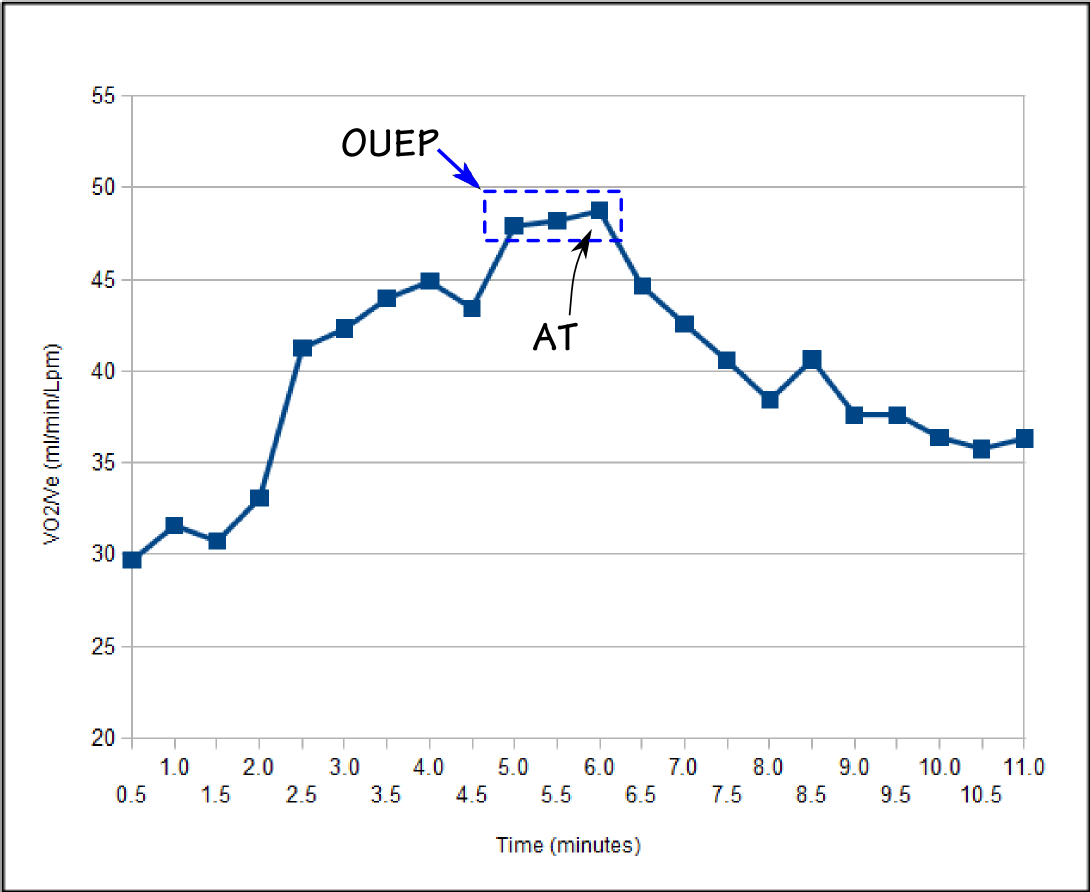
A small group of investigators has proposed that an alternate measurement, Oxygen Uptake Efficiency Plateau (OUEP) has a better correlation with an individual’s cardiac status. During exercise, before the anaerobic threshold occurs, there is a period where a plateau in VO2/Ve occurs. OUEP is the average value of VO2/Ve during this plateau.
The reference equation for OUEP (in ml/min/liter/min) for males is:
39.16 – (0.189 x age) + (0.036 x height (cm))
and for females it is:
42.18 – (0.189 x age) + (0.036 x height (cm))
Although they are calculated from similar values, OUEP and OUES seem to be sensitive to different aspects of cardiopulmonary fitness. Because OUES correlates with maximum VO2 it is increased when an individual is exceptionally fit. OUEP on the other hand, is relatively independent of fitness and appears to decrease only when cardiac disease is present. A study of mortality and morbidity in patients with cardiac disease showed an increased morbidity when OUEP decreased below 75% of predicted and increased mortality when it decreased below 67% of predicted.
Even though OUES has been studied since the mid-1990’s, it has not entered into common use. Part of the reason for this is that even though reference equations for OUES have been available since 2000 almost all studies of OUES have instead used group or longitudinal comparisons. I don’t think that OUES can be used as a substitute for maximum VO2 but in a sub-maximal CPET I think there is enough evidence in its favor that it should be possible to use it as an indication of what the maximum VO2 would have been if the test was adequate. OUEP is a much more recent arrival and at the moment I’d say that the jury is still out on it. The evidence appears to be strongly in its favor however, and if I see that it is reduced I will look carefully at the other CPET values that correlate with cardiac disease.
OUES and OUEP both look to be promising and useful additions to the CPET analysis toolbox. Their great advantage is that they can be calculated from sub-maximal test results. Like many other CPET values however, they are dependent on cardiac output, ventilation-perfusion matching and peripheral oxygen extraction. I suspect that OUES and OUEP will be shown to have limited value when lung diseases like ILD and COPD with diffusion defects are present. For this reason, until they have been studied more extensively with pulmonary diseases, the utility of OUES and OUEP will have to continue to remain on probation and should be relied on only when SaO2 remains normal during testing.
References:
Arena R, Arrowood JA, Fei DY, Helm S, Kraft KA. Maximal aerobic capacity and the oxygen uptake efficiency slope as predictors of large artery stiffness in apparently healthy subjects. J Cardiopulm Rehabil Prev 2009; 29(4): 248-254.
Baba R, Tsuyuko K, Kimura Y, Ninomiay K, Aihira M, Ebine K, Tauchi N, Nishibata K, Nagashima M. Oxygen uptake efficiency slope as a useful measure of cardiorespiratory function reserve in adult cardiac patients. Eur J Appl Physiol 1999; 80: 397-401.
Baba R, Nagashima M, Goto M, Nagano Y, Yokota M, Tauchi N, Nishibata K. Oxygen uptake efficiency slope: a new indec of cardiorespiratory functional reserve derived from the relation between oxygen uptake and minute ventilation during incremental exercise. J Am Coll Cardiol 1996; 28: 1567-1572.
Baba R. The oxygen uptake efficiency slope and its value in the assessment of cardiorespiratory functional reserve. CHF 2000; 6: 256-258.
Baba R, Tsuyuki K, Yano H, Ninomiya K, Ebine K. Robustness of the oxygen uptake efficiency slope to exercise intensity in patients with coronary artery disease. Nagoya J Med Sci 2010; 72: 83-89.
Davies LC, Wensel R, Georgiadou P, Cicoira M, Coats AJS, Piepoli MF, Francis DP. Enhanced prognostic value from cardiopulmonary exercise testing in chronic heart failure by non-linear analysis: oxygen uptake efficiency slope. Eur Heart J 2006; 27: 684-690.
Hollenberg M, Tager IB. Oxygen uptake efficiency slope: an index of exercise performance and cardiopulmonary reserve requiring only submaximal exercise. J Am Coll Cardiol 2000; 36(1): 194-201.
Mollard P, Woorons X, Antoine-Jonville S, Jutland L, Richalet JP, Favret F, Pichon A. Oxygen uptake efficiency slope in trained and untrained subjects exposed to hypoxia. Resp Physiol & Neurobiol 2008; 161: 167-173.
Pogliaghi S, Dussen E, Tarperi C, Cevese A, Schena F. Calculation of oxygen efficiency slope based on heart rate reserve end-points in healthy elderly subjects. Eur J Appl Physiol 2007; 101: 691-696.
Sun XG, Jansen JE, Stringer WW. Oxygen uptake efficiency plateau best predicts early death in heart failure. Chest 2012; 141(5): 1284-1294.
Sun XG, Hansen JE, Stringer WW. Oxygen uptake efficiency plateau: physiology and reference values. Eur J Appl Physiol 2012; 112: 919-928.
Thomson SD, Peacock AJ, Johnson MK. The relationship between oxygen uptake efficiency slope and peak oxgen update is constant across different groups of pulmonary hypertension. Amer J Resp Crit Care 2013; 187: A4679.
Van Laethem C, Bartunek J, Goethals M, Nellens P, Andries E, Vanderheyden M. Oxygen uptake efficiency slope, a new submaximal parameter in evaluating exercise capacity in chronic heart failure patients. Am Heart J 2005; 149: 175-180.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.