Last week I was discussing the use of DL/VA to differentiate between the different causes of gas exchange defects with a physician. DL/VA is DLCO divided by the alveolar volume (VA). It is an often misunderstood value and the most frequent misconception is that it is a way to determine the amount of diffusing capacity per unit of lung volume (and therefore a way to “adjust” DLCO for lung volume). This is not the case because dividing DLCO by VA actually cancels VA out of the DLCO calculation and for this reason it is actually an index of the rate at which carbon monoxide disappears during breath-holding.
[Note: The value calculated from DLCO/VA is related to Krogh’s constant, K, and for this reason DL/VA is also known as KCO. The term DL/VA is misleading since the presence of ‘VA’ implies that DL/VA is related to a lung volume when in fact there is no volume involved. The use of the term DL/VA is probably a major contributor to the confusion surrounding this subject and for this reason it really should be banned and KCO substituted instead.]
I’ve written on this subject previously but based on several conversations I’ve had since then I don’t think the basic concepts are as clear as they should be.
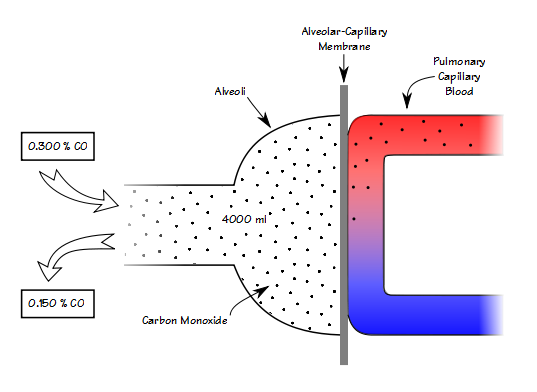
When you know the volume of the lung that you’re measuring, then knowing the breath-holding time and the inspired and expired carbon monoxide concentrations allows you to calculate DLCO in ml/min/mmHg. When you remove the volume of the lung from the equation however (which is what happens when you divide DLCO by VA), all you can measure is how quickly carbon monoxide decreases during breath-holding (KCO).
Continue reading