For the first dozen or so year that I worked in a pulmonary function lab it was with counter-weighted, volume-displacement water-seal spirometers more or less like this:
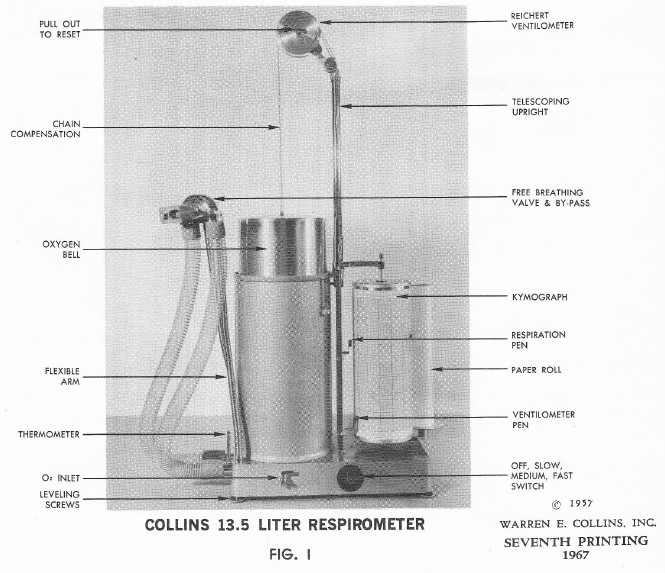
Patients would do a series of tests and I’d end up with a bunch of pen traces on kymograph paper that I’d have to measure with a ruler and use a desktop calculator (it was about a foot square, weighed a couple of pounds and had a nixie tube digital display) to create a hand-written report. I’m not going to suggest that these spirometers were in any way better than what we’re using now but I have to say that I would have seen the following problems more or less immediately.
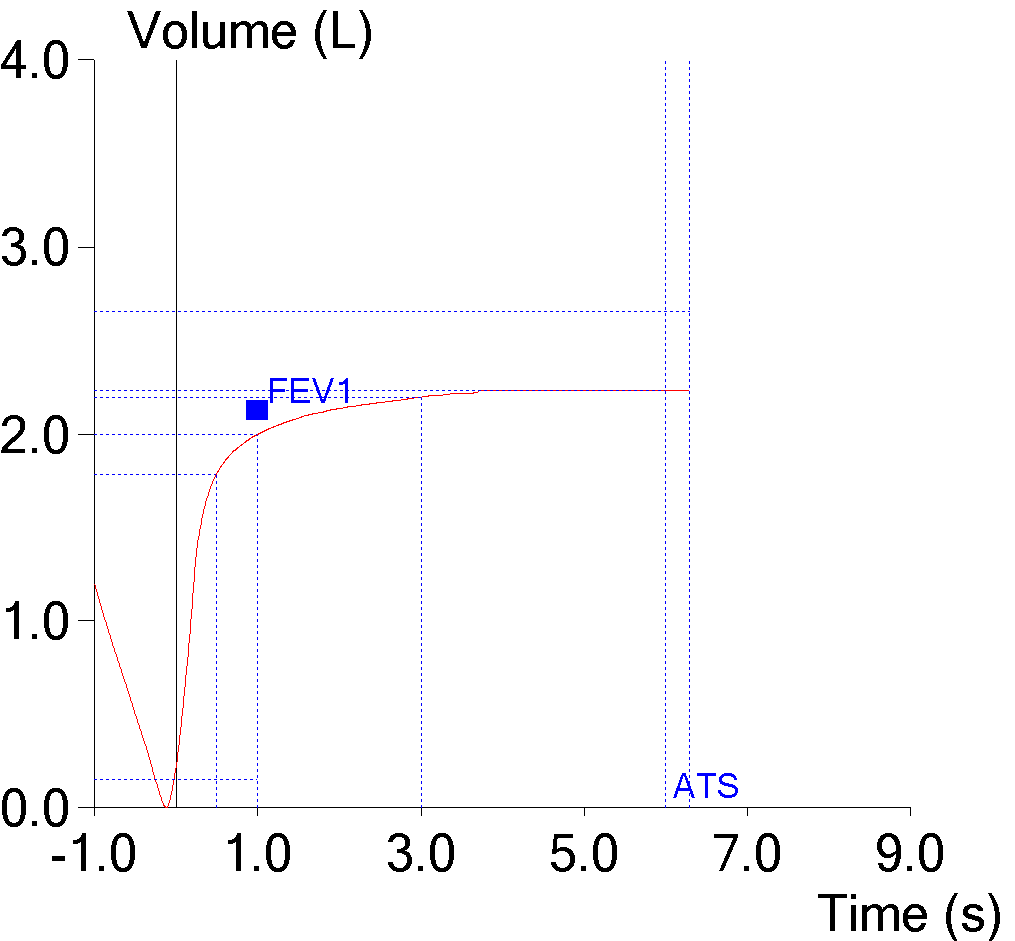
Recently I was reviewing a report from a patient with very severe obstruction and noticed something a bit off about the flow-volume loop. Specifically, the end-exhalation of the tidal loop looked like it was at a significantly higher volume than the end of the FVC effort.
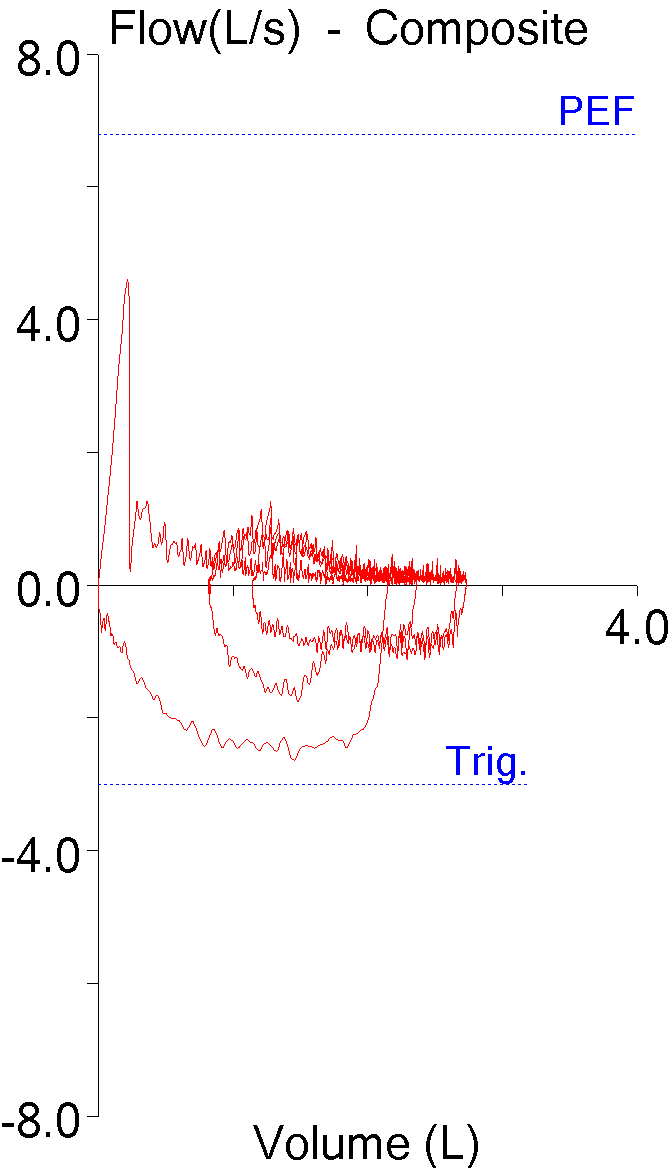
Because the high-frequency sawtooth pattern (from the patient, not the equipment) makes it a little hard to see if this is what was really happening, I downloaded the raw data and re-graphed the volume-time curve with a spreadsheet.