A low FEV1/VC ratio is the primary indication for airway obstruction.
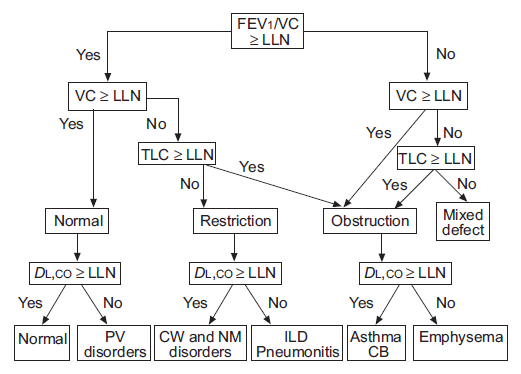
From ATS/ERS Interpretive Strategies for Lung Function tests, page 956.
The ATS/ERS statement on interpretation says
“The VC, FEV1, FEV1/VC ratio and TLC are the basic parameters used to properly interpret lung function (fig. 2). Although FVC is often used in place of VC, it is preferable to use the largest available VC, whether obtained on inspiration (IVC), slow expiration (SVC) or forced expiration (i.e. FVC).”
I understand and in general agree with the idea of using the largest VC regardless of where it comes from and this is because the FVC is often underestimated for any number of good (and not so good) reasons. When this happens the FEV1/FVC ratio will be overestimated and airway obstruction will be under-diagnosed. However the ATS/ERS statement is also grounded in the notion that all vital capacities (FVC, SVC, IVC) are the same and this isn’t necessarily true. The problem comes from the fact that the predicted values and lower limit of normal (LLN) for the FEV1/VC ratio always come from reference equations for FEV1/FVC ratios. Because the SVC (and IVC) are usually larger than the FVC this means there is at least the potential for airway obstruction to be over-diagnosed.