From a Fenyves & Gut sales brochure kindly provided by Emanuele Isnardi.
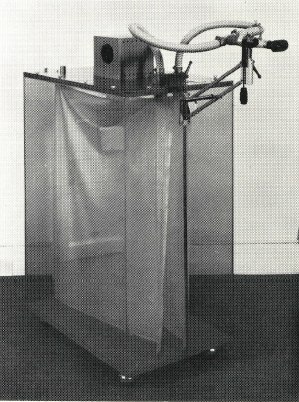
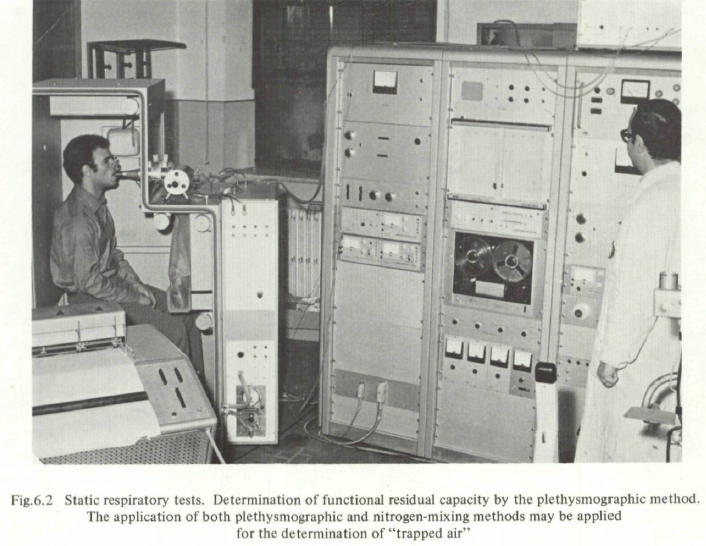
“Principle of measurement: the patient breathes room air (or, in special cases, a gas mixture) through a sterilisable, heated pneumotachograph head fitted to a mouthpiece of breathing mask. The resulting pressure different of a few millimetres water gauage picked up the the pneumotachotraph and proportional to the flow V is concerted to the corresponding positive and negative voltages by means of a pressure transducer and registered in an electronic integrator after amplification. The voltage resulting from this operation is proportional to the tidal volume (TV). The factor of the proportional relationship is determined by volumetric calibration, using a calibration pump. One litre of air is pumped through the pneumotachograph head, which is pre-heated to operating temperature. This is the only reasonable method of checking the entire system. A balance control compensates for any lack of symmetry between pneumotachograph heads.
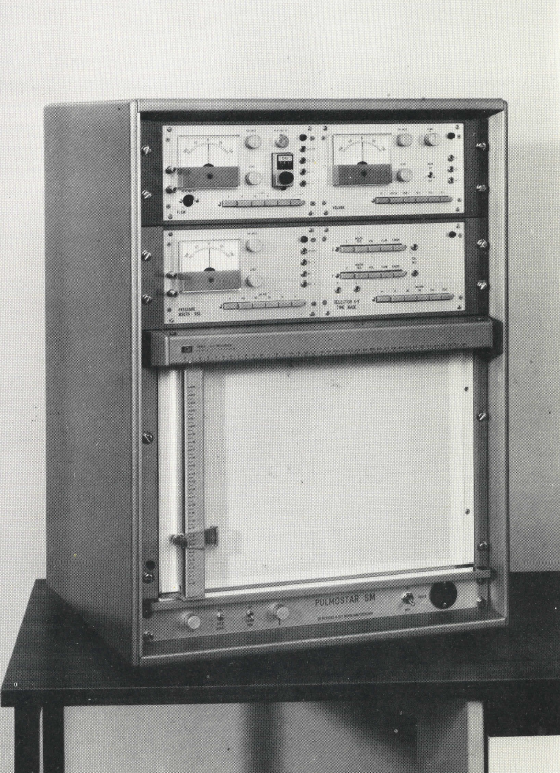
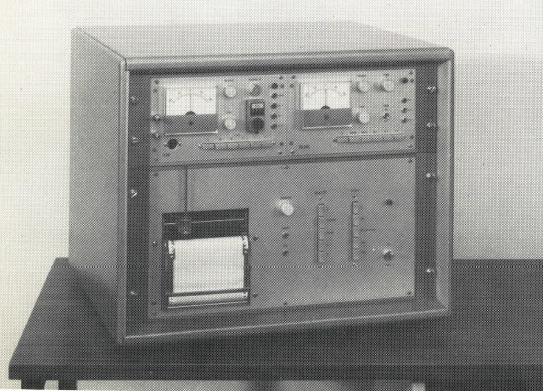
The S basic unit this consists of a slide-in unit for measuring the flow and a linked integrator and calibrating device. Measurements ranges: 1, 2, 5, 10, 20 litres or litres/sec., respectively, on full-scale deflection; time constants: 1000, 20 , 10, 5 seconds. Push-button selectors. Automatic marking of zero-flow pointes V=0; heating of pneumotachograph head; data output using optional built-in single- or multi-channel compensated direct recordes or X-Y records; repectively.
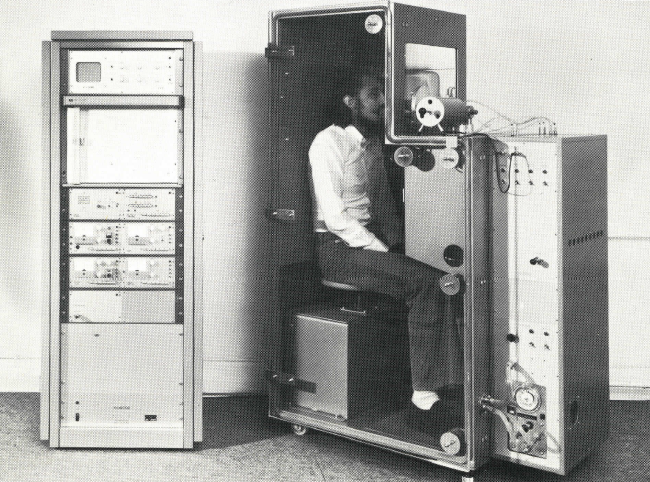
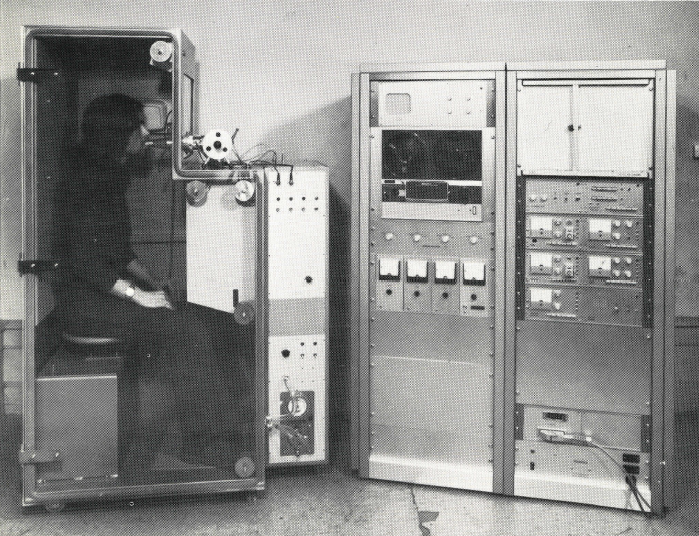
Determinable parameters at rest and during exercise: tidal volume TV, inspiratory reserve volume IRV, expiratory reserve volume ERV, inspiratory capacity IC, forced inspiratory volume FIV, vital capacity VC, forced vital capacity FVC, forced expiratory volume FEV1, percentage expired %FEV1/VC and %FEV1/FVC, mean inspiratory flow MIFR, mean expiratory flow rate MEFR, mean flow rate MFR, peak inspiratory flow PIFR, peak expiratory flow rate PEFR, peak flow rate PFR, forced inspiratory flow FIF, forced expiratory FEF, forced mid-expiratory flow rate FMF, minute volume MV, maximum breathing capacity MBC, indirect maximum breathing capacity IMBC, maximum voluntary ventilation MVV, excess exercise ventilation EEV, standardised ventilation SV, ventilation in response to exercie VRE, respiratory frequency F, duration of inspiration, and expiration, respectively, flow-volume diagram also with He2 (X-Y recorder necessary).”