The European Respiratory Society has just published the first standards for DLNO testing. This is a signal that DLNO is moving from a research setting into routine clinical testing. Although it is unlikely that most PFT labs will immediately jump into DLNO testing, the standard is still interesting because of an extensive discussion of DLNO, DLCO, DMCO and Vc measurements and physiology. The DLNO standards (and their supplementary material) are open-access and can be downloaded from the European Respiratory Journal.
DLNO is performed in the same manner as a single-breath DLCO and it is specifically recommended that DLCO and DLNO tests be performed simultaneously. There are however, specific test system requirements based both on the properties of NO and on the two types of NO analyzers:
- Nitric Oxide reacts with oxygen to form NO2 and at the levels used for DLNO testing (40-60 ppm) does so at a rate of approximately 1.2 ppm per minute. DLNO test gas is therefore usually stored as 400-1200 ppm NO in N2 and mixed into the DLCO test gas mixture (0.3% CO, 21% O2) ≤2 min before the DLCO/DLNO test. This would seem to require that the DLCO/DLNO test gas mixture to be held in a reservoir of some kind and to preclude the use of a demand valve but this was not specifically discussed. Because of uncertainties that occur when mixing the DLCO/DLNO gas mixture and in how long the mixture may be held in the reservoir the inspired NO concentration must also be measured immediately before the DLCO/DLNO test is performed.
- The type of NO gas analyzer will determine how the expiratory gas concentrations are measured. Chemiluminescent analyzers usually have a response time on the order of ≤70 msec, and for these reasons can be used to perform a real-time analysis of exhaled air. Chemiluminescent analyzers are expensive however, and can add significantly to the cost of a test system. Electrochemical cells are significantly less expensive but have a response time on the order of 10 seconds and are therefore suitable only to test systems that mechanically collect an alveolar sample.
- Breath-holding times of between 4 and 10 seconds have been used in DLNO research. The DLNO standard notes that breath-holding time affects the measurement of DLNO and DLCO, particularly when a ventilation inhomogeneity is present. In particular it was noted that shorter breath-hold times tended to overestimate DLCO and underestimate VA. However, it also has been noted that the exhaled NO concentration is approximately 5% of the inspired concentration after a 5 second breath-hold and 1% after a 10 second breath-hold. Electrochemical NO analyzers are less sensitive (a resolution of approximately 0.5 to 1.0 ppm) than chemiluminescent analyzers (which have a resolution of 0.5 ppb). For this reason the DLNO standards recommend that a 4-6 second breath-hold period be used with electrochemical NO analyzers whereas a 10 second breath-hold can be used with chemiluminescent analyzers.
- If DMCO and Vc are being calculated the expired alveolar O2 concentration must be measured so that 1/θCO can be calculated.
The standards for CO and NO analyzer linearity, accuracy and drift are essentially identical to those of the 2017 DLCO standards. The same applies for flow and volume accuracy and the need for daily volume calibrations. Recommendations that differ to one extent or another from the 2017 DLCO standards are:
- The gas analyzers should be zeroed before each test and the zero should be re-measured after the test. Results should be adjusted for any drift. The inspired NO concentration should be measured just before the test.
- A VA measurement check by performing a DLCO/DLNO test using a calibration syringe pulled back to the 1 liter mark is recommended. VA should be between 2.7 and 3.3 liters with the syringe dead space substituted for anatomical dead space. At the same time DLCO should be <0.5 ml/min/mmHg and DLNO should be <3.0 ml/min/mmHg.
- Hemoglobin correction for DLNO results is not recommended but corrections in DLCO for hemoglobin and COHb remain the same.
- Biological QC should be performed weekly. Differences from prior mean values should be ≤5.0 ml/min/mmHg for DLCO and ≤20.0 ml/min/mmHg for DLNO.
- The CO, NO and insoluble gas (He, CH4, Ne) analyzers should be tested monthly for linearity using serial dilutions of know gas concentrations.
Patient preparation and the DLNO testing maneuver is identical to that of the DLCO. Measuring the breath-holding period using the Jones-Meade approach is recommended. Washout and alveolar volumes are also the same as for DLCO testing. Intra-session and inter-session repeatability and reproducibility for DLCO appears to be slightly less stringent than for the 2017 DLCO standards but this may be partly due to the range of acceptable breath-holding times (5-10 seconds) for DLNO testing.
Roughton and Forster’s work on DLCO in the 1950’s showed that diffusing capacity was a series resistance with a membrane component and a blood component:
![]()
Where:
DMCO = alveolar-capillary membrane conductance
Vc = pulmonary capillary blood volume
θCO = rate at which CO is taken up by red blood cells
Early work showed that in normal subjects DLNO is approximately 5 times larger than DLCO. This is partly due to the fact that the difference in tissue diffusivity of NO is 1.97 times that of CO and because the reaction rate of NO with hemoglobin is approximately 1500 times faster than CO. In addition because NO does not compete for O2 binding sites on hemoglobin NO uptake is mostly independent of FiO2. In a sense DLNO is not excessively high, DLCO is low mostly because CO uptake is highly dependent on the pulmonary capillary blood volume and the alveolar oxygen concentration. NO uptake is however, more dependent than CO uptake is on alveolar surface area and lung volume.
Clinically DLNO is primarily related to membrane conductance and DLCO is primarily related to Vc. For this reason, the most common way of expressing the differences in these measurements for a given individual is the DLNO/DLCO ratio. Decreases in the DLNO/DLCO ratio tend to correlate with decreases in membrane conductance and/or increases in pulmonary capillary blood volume whereas increases in the DLNO/DLCO ratio correlate with increases in membrane conductance and/or decreases in pulmonary capillary blood volume.
In the early stages of COPD the DLNO/DLCO ratio has been shown to rise, while in established COPD the ratio appears relatively normal (although both DLNO and DLCO are reduced). In Cystic Fibrosis the DLNO/DLCO ratio is reduced. A reduced DLNO/DLCO ratio has also been shown in Sarcoidosis. Elevated DLNO/DLCO ratios have been found in hepatopulmonary sundrome and heart failure.
In many ways the clinical use of DLNO and the DLNO/DLCO ratio is still in its early stages and comparison between different studies is made more difficult because different DLNO measurement techniques have often been used. The DLNO standard itself notes:
“…disease-specific patterns of DLNO and DLCO, DLNO/DLCO and Vc will remain imprecise until more clinical studies are reported using a standardised technique.”
A set of DLCO and DLNO reference equations was developed from the data of four different studies but was not presented within the standards. They were however, included in a supplementary materials spreadsheet that was designed to calculate the percent predicted DLCO, DLNO, DMCO and Vc from test results. From this spreadsheet the DLNO reference equations are:
DLNO (Male) = (0.81 x height (cm)) – ((0.01 x (age2)) + 44.1
DLNO (Female) = (0.81 x height (cm)) – ((0.01 x (age2)) + 9.7
You can’t discuss DLNO testing without also discussing DMCO and Vc and this is because for a variety of reasons DLNO was initially considered to be DMCO * 1.97 (where 1.97 is the ratio of tissue diffusivity for NO compared to CO) or at least so close an approximation that any differences could be ignored. This however, depended on the assumption that the rate of NO uptake was close to infinite. Subsequent research has shown this to be incorrect and that θNO is approximately 4.5 ml/ml blood/min/mmHg.
As an interesting side note, a finite NO uptake rate also implies DMCO is significantly underestimated when measured by the traditional Roughton & Forster technique that consists of serial DLCO measurements at different FiO2’s and where DMCO is considered to be the intercept of a line plotted using 1/DLCO versus θCO (where θCO depends on FiO2). This may well be because hemoglobin has sites for 4 oxygen molecules and the FiO2’s chosen are almost always within the normal physiological range where there is at most one binding site available. Lower FiO2’s where multiple binding sites are available may well cause the 1/DLCO vs θCO line to become a curve. For this reason, although DLNO is not DMNO, DMNO is most probably equal to DMCO x 1.97.
Using realistic values for θNO and θCO it is possible however, to calculate DMCO and Vc from DLNO and DLCO. Specifically:
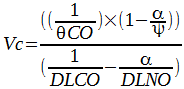
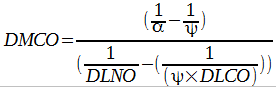
Where:
а = 1.97
1/θCO = (0.0062 x PAO2 + 1.16) x (Ideal Hgb / measured Hgb)
Ψ = θNO/θCO = 8.01
The publication of a standard for DLNO testing is welcome for any number of reasons. In particular DLNO provides another viewpoint concerning gas exchange in the lung. Regardless of whatever interest level there may or may not be in DLNO testing the 2017 DLNO standard’s discussion of gas exchange physiology was both interesting and helpful in understanding DLCO, DMCO and Vc. At present the effect that different lung disorders have on DLNO and the DLNO/DLCO ratio aren’t overwhelmingly clear but I expect that this will improve now that a standardized technique is available. In addition the standard’s consensus statement about 1/Θ for CO, although potentially controversial, is a welcome update in this area of study.
One of the barriers towards the routine performance of clinical DLNO testing is that at the present time none of the major PFT equipment manufacturers in the USA offer DLNO testing systems. In addition there are no CPT codes for it yet which means that it’s not possible to bill a patient’s insurance for a DLNO test. However, since the DLNO standard advocates combined DLCO and DLNO testing there is no reason that at least the DLCO component can’t be billed.
One minor criticism of the DLNO standard is that I would like to have seen more discussion of the differences in how NO and CO are taken up by hemoglobin, in particular the reason for the different speeds at which this occurs. I also did not see any mention of the fact that the absorption of NO creates methemoglobin. The concentrations of NO used in DLNO testing are too low for this to be a safety issue, even with repeated testing, but I think it is an important physiological consideration.
An additional criticism is that existing electrochemical NO analyzers were approved for DLNO testing. Their low sensitivity and resolution requires a shorter breath-holding period and this biases both DLNO and DLCO results. I am not against electrochemical anlyzers per se but I do think that the specifications for DLNO testing should have been set with test quality and inter-lab reproducibility in mind. The use of somewhat different test standards for electrochemical and chemiluminescent analyzers creates the potential for DLNO and DLNO/DLCO results to be different depending on which technology is used to measure them.
Realistically though, the 2017 standards did an excellent job of addressing most of the issues surrounding DLNO testing and I commend its authors for providing a good foundation for future DLNO testing.
Note: A discussion of the physiology of DLNO testing was previously posted in DLNO isn’t the same as DMCO but sometimes it’s useful to pretend it (almost) is.
References:
Zavorsky GS, Hsia CCW, Hughes JMB, Borland CDR, Guenard H, van der Lee I, Steenbruggen I, Naeije R, Cao J, Dinh-Xuan AT. Standardisation and application of the single-breath determination of nitric oxide uptake in the lung. Eur Respir J 2017; 49: 1600962.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
Hi, the DLNO prediction equations are located in Table 2 of the ERS Task force document (page 11), so they are presented within the paper.
Thanks. My bad. Looked right at them and didn’t see them.
As well, there is some good argument that the DLNO should replace the DLCO due to its technical and physiological superiority compared to DLCO. I encourage the reader to view this article: http://www.sciencedirect.com/science/article/pii/S1569904816302816
Dr. Zavorsky –
I’d say that DLNO and DLCO have different strengths and weaknesses and that it will probably be most useful for them to be compared rather than taken individually. I’d also say that the clinical studies of DLNO are still in their early stages and the 2017 standard will do much to improve this by giving us the ability to meaningfully compare studies of DLNO and their related DLCO counterparts. It’s also going to be a while before DLNO has the market penetration that DLCO testing has, so regardless of DLNO’s technical superiority DLCO is going to be around for some time to come.
Regards, Richard