I was reviewing a spirometry report and noticed something odd about the flow-volume loop, or more specifically the tidal loop, and this got me to thinking about what tidal loops can tell us about test quality, patient physiology and the ability of the technician to coach a spirometry test.
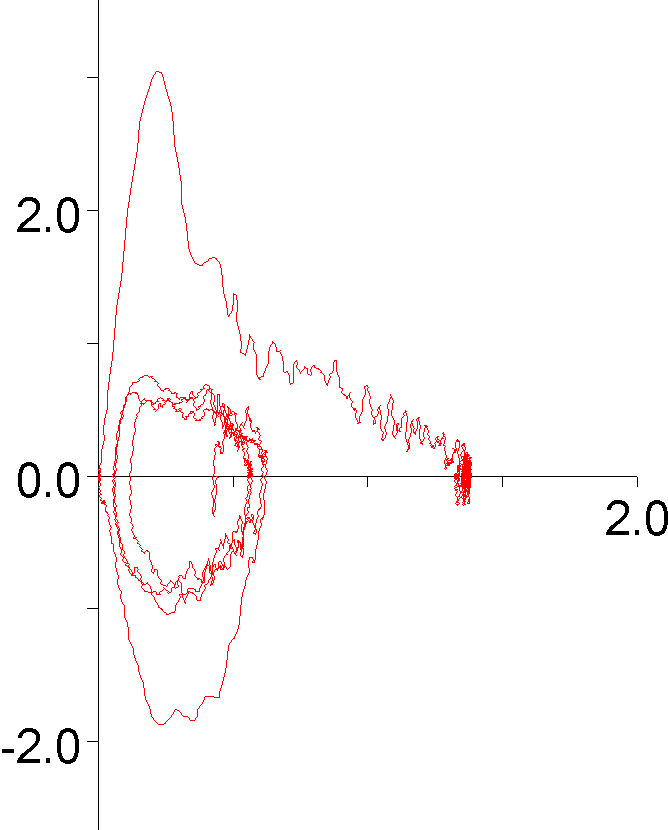
There are at least a couple things wrong with this FVC test effort. First the exhalation time was only about 3 seconds so the FVC volume was likely underestimated by a fair amount. Second, it wasn’t reproducible and this was actually the patient’s the best test effort. What I noticed however, was that the tidal loop was shifted almost completely to the left.
There are a number of criteria for assessing the quality of a forced vital capacity. Exhalation quality can be determined reasonably well by back extrapolation, expiratory time and the terminal expiratory flow rate. When it comes to assessing the completeness of the inspiration that precedes the exhalation however, there really isn’t much to go on other than the reproducibility of an individual’s spirometry efforts.
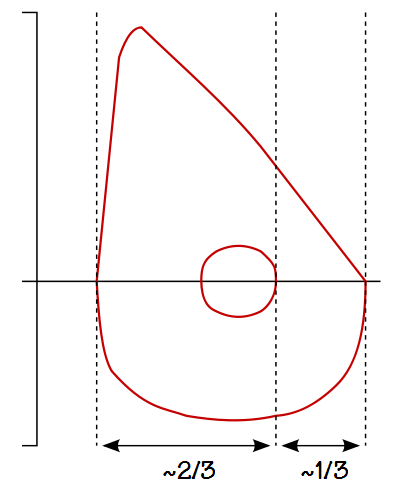
When I measured the tidal loop what I saw was that IRV was about 0.10 L and the ERV, although likely underestimated by a fair amount, was at least 0.80 L. What I actually think this tidal loop is saying is that the patient didn’t take as deep a breath as they could at the start of the test, but what other things could affect the position of the tidal loop?
For an individual with normal lungs, the IC is usually around twice the volume of the ERV.
Body weight can affect the position of the tidal loop. Because of the compressive effect an increase in body weight has on the thorax FRC tends to decrease when BMI increases. This moves the tidal loop closer to RV, thereby increasing IC and decreasing ERV. A low body weight has somewhat the opposite effect and FRC tends to increase slightly as BMI decreases.
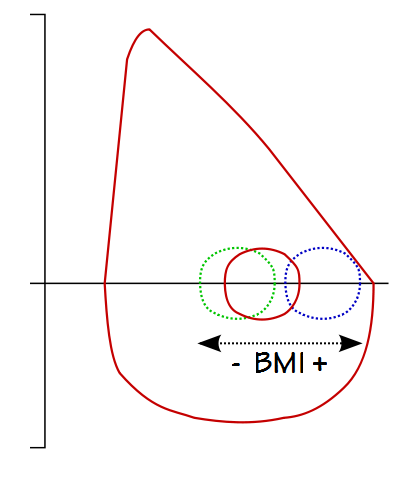
Not all individuals with tidal loops shifted rightwards towards RV are overweight, but many individuals that are overweight will have a rightwards shifted tidal loop. In this instance at least, the position of the tidal loop says something about an individual’s physiology.
Regardless of an individual’s BMI however, a rightwards-shifted tidal loop means that tidal breathing is occurring where an expiratory flow limitation is more likely. In addition because it is on a less favorable portion of the pressure-volume curve, the work of breathing is higher when tidal breathing is near RV and these may be a factors in some patients’ sensation of dyspnea.
The expiratory flow limitation that accompanies severe COPD causes gas trapping and hyperinflation. FRC increases, IC decreases and the tidal loop tends to shift leftwards toward TLC.
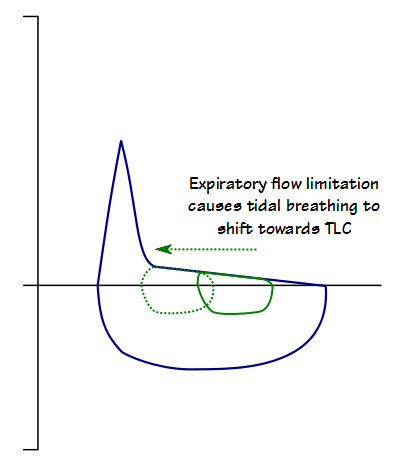
The leftwards shift that is due to airway obstruction is often offset by a decrease in FVC which can keep the tidal loop more or less centered until the obstruction is extremely severe. Regardless, when tidal breathing is shifted towards TLC it is also on an inefficient portion of the pressure-volume curve of the lung. The elevated work of breathing and limited ability to increase tidal volume are factors that increase dyspnea in patients with COPD.
Spirometry has a psychological as well as a physiological aspect. The maneuvers required for the correct performance of a spirometry effort are often not familiar to patients and for this reason they often need coaching. An important aspect of a PFT technician’s job therefore, is to properly lead a patient through testing and this also means cuing them at the right time.
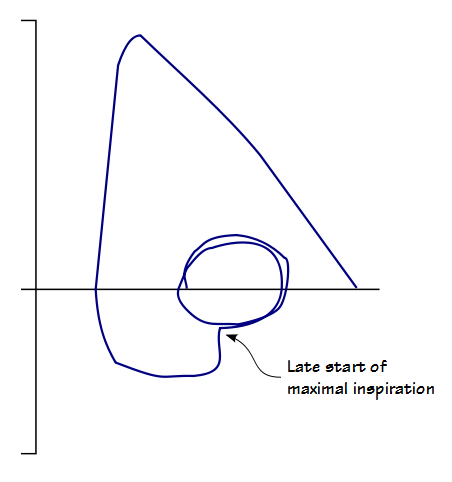
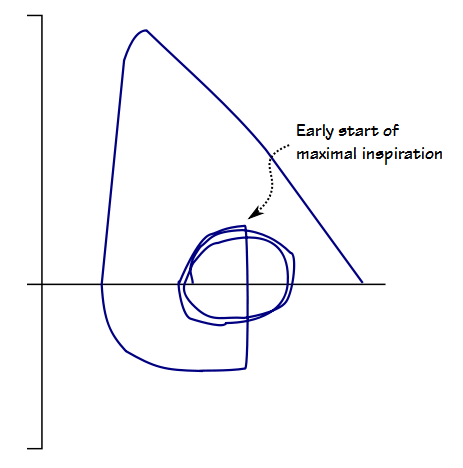
When a patient is cued at the wrong time they can be unprepared to take a full inspiration and the quality of the effort can be reduced. Noting where the full inspiratory effort began can be a clue about how well a technician is coaching patients, particularly when it occurs in more than one test effort and more than one patient.
The tidal loop is often unnoticed and underutilized. Tidal loops can be shifted rightwards toward RV because of obesity and leftwards towards TLC because of airway obstruction. A tidal loop that is shifted towards RV or TLC when neither of these conditions is present may in fact be giving us an important diagnostic clue or a clue about test quality instead.
There are no ATS/ERS criteria for the tidal loop and attempts in the past to use the tidal loop diagnostically have been largely unsuccessful because tidal breathing is often inconsistent and irreproducible. There are also good reasons why IC and ERV are measured from a slow vital capacity maneuver instead of a forced vital capacity. This doesn’t mean that a tidal loop can’t provide additional information about the patient.
The spirometry efforts from my lab and from several other labs I am familiar with usually contain one or more tidal breaths. I was reminded that this is not a given however when I reviewed a report shown to me by a friend that not only had no tidal loops but no inspiratory loops either. When I took a close look it was evident from the way the graphic was formatted that is was in fact only possible for the expiratory flow-volume curve to be shown. I will agree that FEV1, FVC, Peak Flow, and the FEV1/FVC ratio all come from the expiratory part the spirometry maneuver and I can understand why a manufacturer or lab might want to simplify a spirometry report but I think it is a mistake to exclude not only the inspiratory flow-volume loop but the tidal loops as well. We need every clue we can get.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License