Oddly enough, I recently got a couple emails on the same day about the FEF25-75 and ended up corresponding for a while with the authors. FEF25-75 is a subject that somehow manages to keep resurrecting itself no matter how many stakes have gotten hammered into its heart. My opinion (expressed previously), and those of many others, is that the measurement of FEF25-75 is overly affected by FVC volume and expiratory time; that its reproducibility is poor; that its “normal” range is too broad to be meaningful; and that the FEF25-75 is usually only abnormal when the FEV1 is also below the LLN. Despite all this the FEF25-75 still continues to be used by many clinicians and researchers.
While discussing it however, one of the points that came up was how the “best” FEF25-75 should be selected. Given that it’s not clear to me exactly what the FEF25-75 is measuring, I am not sure there is such a thing as a “best” FEF25-75. Out of curiosity I reviewed a number of the older studies concerning FEF25-75 and although all the studies stated that their subjects performed multiple spirometry efforts I was interested to note that the FEF25-75 selection process was rarely, if ever, detailed. Of the exceptions, one stated the FEF25-75 was taken from the spirometry effort with the best FEV1 and another stated that the FEF25-75 was averaged from three efforts. The ATS/ERS statement on spirometry says that the FEF25-75:
“… is taken from the blow with the largest sum of FEV1 and FVC.”
This makes a certain amount of sense but because this statement is not referenced to any studies it should only be taken as a way to standardize the measurement of the FEF25-75 and not as a resolution about what constitutes the “best” FEF25-75. Even so it still leaves the door open to some varied interpretations. There are at least two situations where this is problematic. First, when two spirometry efforts have the same combined FVC + FEV1 value, and second, when an individual’s spirometry efforts are highly variable and the FVC and FEV1 have to be selected from separate efforts.
I didn’t have to go very far to find examples for both of these problems.
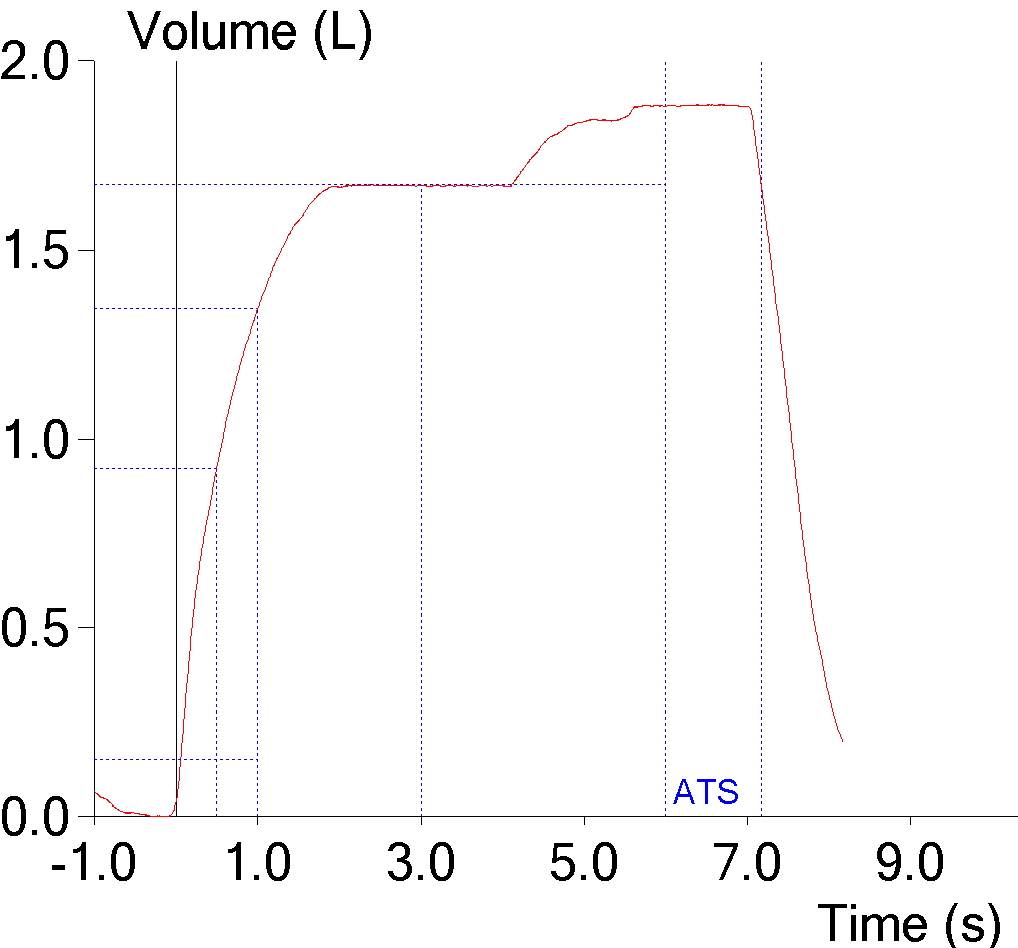
| Effort #1: | Effort #2: | |
| FVC: | 2.03 | 1.97 |
| FEV1: | 1.00 | 1.06 |
| FEV1/FVC: | 49 | 54 |
| FEF25-75: | 0.28 | 0.43 |
This is from an individual with severe airways obstruction and both spirometry efforts (which were far and away the patient’s best) have the same value for FVC+FEV1. The fact that FEF25-75 is sensitive to FVC should be quite clear, since the effort with the largest FVC has a FEF25-75 that is 35% smaller than the effort with the largest FEV1 even though the difference in FVC is only about 3%. In one sense it doesn’t matter which of these is the “best” FEF25-75 since the predicted value for this individual was 2.74 L/sec and both results are severely reduced. In another sense it matters a lot, since whenever the sum of the FEV1 and FVC are the same (or essentially the same) how do you decide which FEF25-75 to use? Best FEV1 or best FVC?
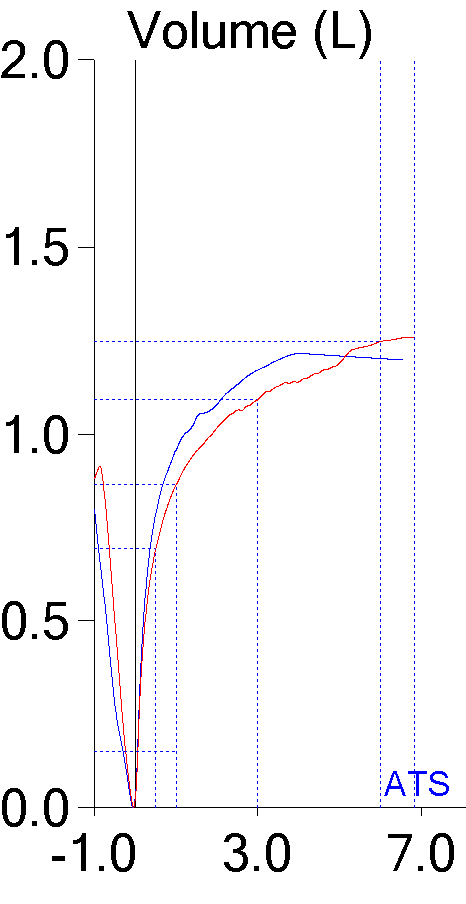
| Effort #1: | Effort #2: | |
| FVC: | 1.17 | 1.28 |
| FEV1: | 0.98 | 0.84 |
| FEV/FVC: | 84 | 66 |
| FEF25-75: | 0.84 | 0.48 |
In this particular instance, the patient had fairly variable efforts. The effort with the best FVC had a low FEV1 and the effort with the best FEV1 had a low FVC. Our standard practice is to combine the efforts and report the best FVC with the best FEV1. Although our software lets us select an FVC from one effort and an FEV1 from another (and will re-calculate the FEV1/FVC ratio accordingly) it only lets us choose the flow-based data (i.e. FEF25-75, MEF50, MIF50 etc) from one effort. So given the discrepancy in test quality, which FEF25-75 should be selected?
In addition, the ATS/ERS statement on interpretation says that the largest VC, regardless of the source, should be used to calculate the FEV1/FVC ratio. So a very related problem is when an SVC or IVC is actually used to re-calculate the FEV1/VC ratio. Since SVC and IVC maneuvers are not timed FEF25-75 cannot be calculated. This means that the only FEF25-75 that can be reported comes from the spirometry effort the FEV1 was taken from.
Finally, and this may not be fair, but what do you do with an FEF25-75 that is selected from the spirometry effort with the best FVC+FEV1 and the test quality is so poor the FEF25-75 is meaningless?
These issues also raises an important question about trending the FEF25-75 and using the changes from one set of tests to another as a guideline for therapy. I doubt that this has been studied specifically but I have to think at least some of the variation in FEF25-75 over time has more to do with the selection process than it does with any clinical changes.
The only standard for selecting an FEF25-75 from multiple efforts is based on FVC and FEV1. This makes a certain amount of sense but does not address the issue of what really constitutes the “best” FEF25-75. Since there is no particular consensus on what the FEF25-75 is really measuring I am not sure that there is such a thing as a “best” FEF25-75, but then I don’t think the FEF25-75 is worth reporting in the first place.
When the FEF25-75 was first reported over 40 years ago, its results were taken as a way to detect small airways disease. Since that time the FEF25-75 has been shown to be a highly variable measurement with relatively poor reproducibility that is markedly affected by FVC volume and expiratory time. The fact that selecting an FEF25-75 from multiple spirometry efforts is itself a variable and idiosyncratic process just adds one more reason not to use it.
References:
Brusasco V, Crapo R, Viegi G. ATS/ERS Task force: standardisation of lung function testing. Standardisation of spirometry. Eur Respir J 2005; 26: 319-338.
Brusasco V, Crapo R, Viegi G. ATS/ERS Task force: standardisation of lung function testing. Interpretive strategies for lung function tests. Eur Respir J 2005; 26: 948-968.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License