When Tiffeneau described the FEV1 in 1947 and Gaensler the timed FVC and FEV1/FVC ratio in 1950 this opened up an entirely new territory for pulmonary investigators to explore. Numerous new measurements were rapidly mapped out with often conflicting titles. The situation became confusing enough that the British Thoracic Society met in 1956 specifically to standardize terminology. At this time only the volume-time curve was available for measurement purposes (usually a pen trace on kymograph paper) and this fact helped determine what measurements it was possible for researchers to make.
These measurements were in somewhat common use for the first decades of modern spirometry. They have since mostly passed into disuse and have largely been forgotten either because they were superceded by the flow-volume loop or because they never established any particular clinical value. Even so most of these measurements are included as reporting options in current spirometry testing systems. Despite being of questionable value they are still interesting if for no other reason than that they highlight the incredible number of ways that a volume-time curve can be analyzed.
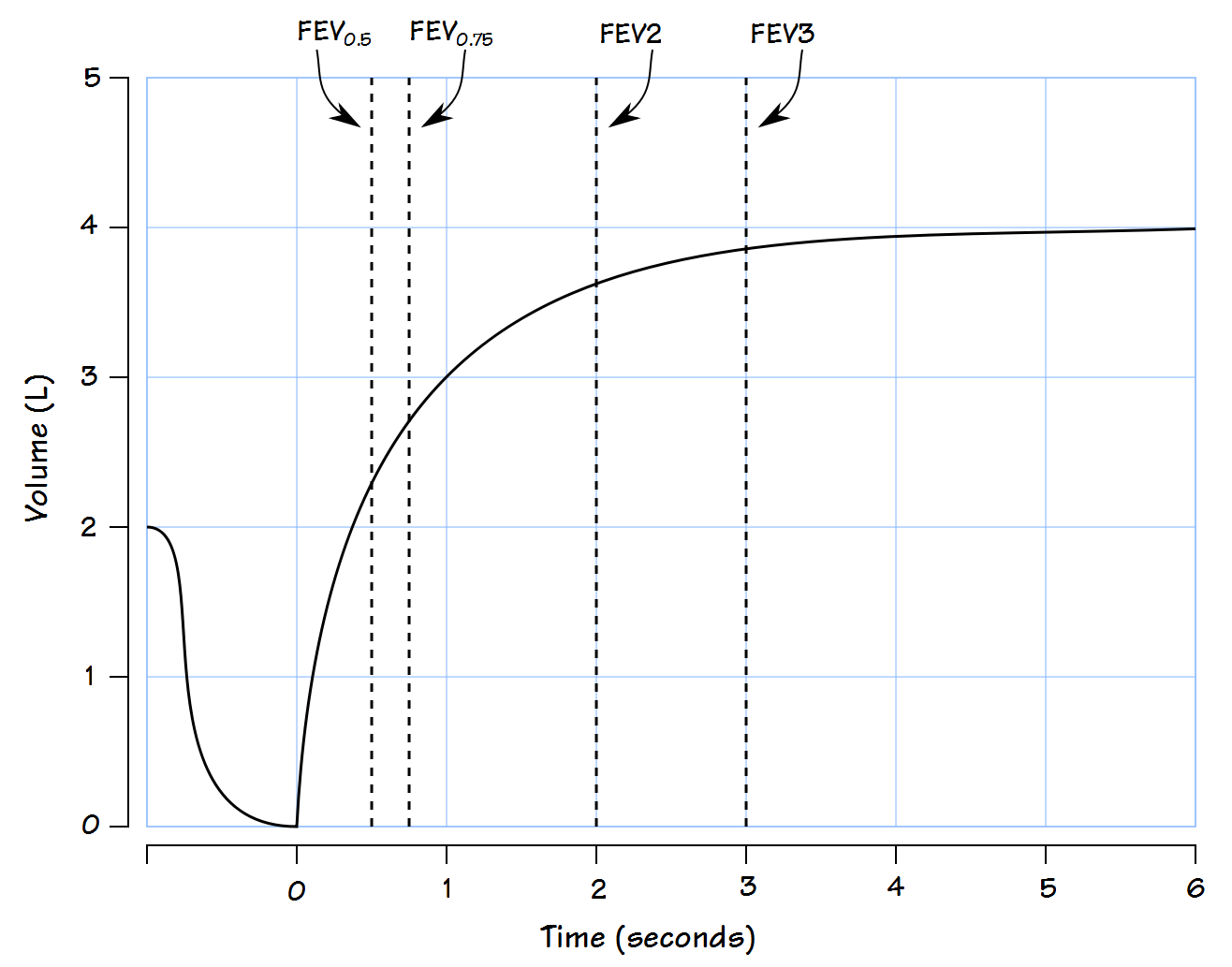
FEV0.5
In retrospect the use of the FEV1 and FEV1/FVC ratio to assess airway function seems inevitable but in the early decades it wasn’t clear what timed measurements were optimal. Like the FEV1 the forced expired volume in 0.5 seconds can be measured from the volume-time curve. The FEV0.5 is considered more reproducible than the Peak Expiratory Flow and has been used to assess cough. Although normal values for the FEV0.5 were included in the reference equations from the 1961 VA-Army and Kunudson’s 1976 spirometry study this measurement has rarely been used in adults but has instead found extensive use when measuring and reporting spirometry in infants and children.
FEV0.75
The FEV0.75 appears to have been used primarily in Britain and Europe. Interestingly it (multiplied x 40) was assessed in terms of normal values for the MVV (MBC) and reference equations for the FEV0.75 were never developed or published. It was actually used relatively rarely even through the 1970’s and was only used as recently as 2000 in a longitudinal study of Finnish smokers because the original study used the FEV0.75.
FEV2, FEV3:
FEV2 and FEV3 have been reported occasionally in articles since the 1950’s. Although normal values for FEV2 and FEV3 were included in Knudson’s 1976 spirometry study these measurements have never been commonly used. One 2005 study proposed estimating the FVC from the FEV2 and FEV3 in cases where the expiratory effort was otherwise short. More recently the FEV3/FVC ratio has been proposed by several authors as a more accurate assessment of small airway function than the FEF25%-75% but although this idea has merit it has not yet achieved common use.
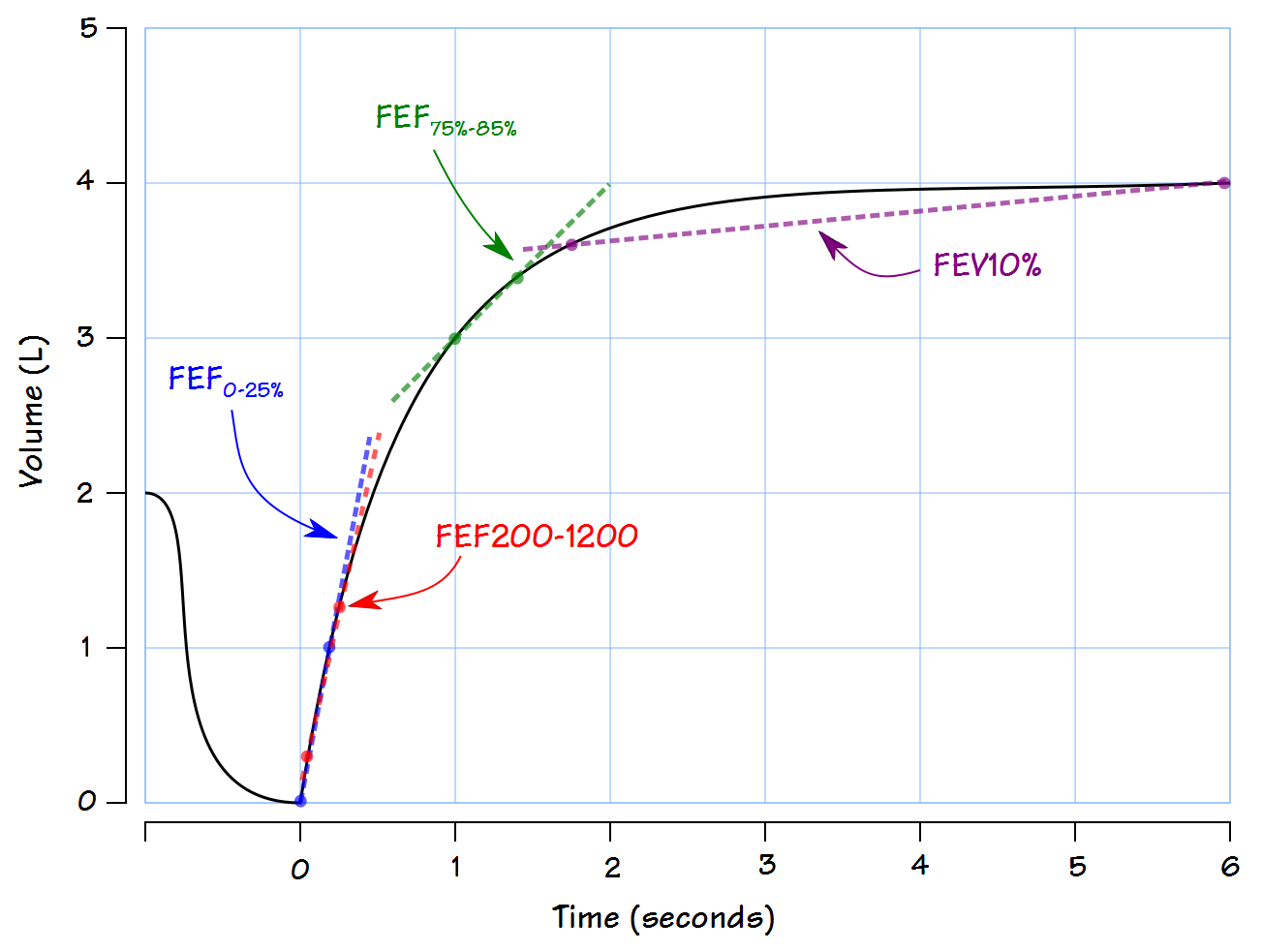
FEF200-1200:
The FEF200-1200 is the average expiratory flow rate between 0.2 and 1.2 liters of the FVC. It was considered as a substitute for Peak Flow and for many individuals there is a relatively close match between the two. Since it is measured across a specific volume however, it becomes progressively less accurate as the vital capacity becomes smaller (either normally as in short or elderly individuals or with restrictive lung disease) or in circumstances where the peak flow occurred over a particularly short interval (commonly seen in COPD).
FEF0-25%
The FEF0-25% is the average flow rate over the first 25% of the FVC. Like the FEF200-1200 is was intended to assess the maximal expiratory flow rate at high lung volumes. Although the Peak Flow usually occurs within the first 25% of the FVC, the FEF0-25% is the average flow rate over that volume, which includes the periods of accelerating and decelerating flow rates and for this reason tends to correlate relatively poorly with peak flow.
FEF75%-85%
The average flow rate from 75% to 85% of the FVC occurs at low (close to RV) lung volumes and for this reason is expected to reflect airflow from the smaller airways. Normal values were first developed by Morris et al in 1975 and were found to correlate with height, age and smoking history. Even more than the FEF25%-75% (discussed previously) however, the FEF75%-85% is highly sensitive to the FVC volume and expiratory time.
FEV10%
The average flow rate during the last 10% of the FVC. Like the FEF25%-75% this value was expected to reflect airflow from the smaller airways. It is also highly sensitive to FVC volume and expiratory time. There are no reference equations and this measurement never appeared in more than a few research articles and textbooks.
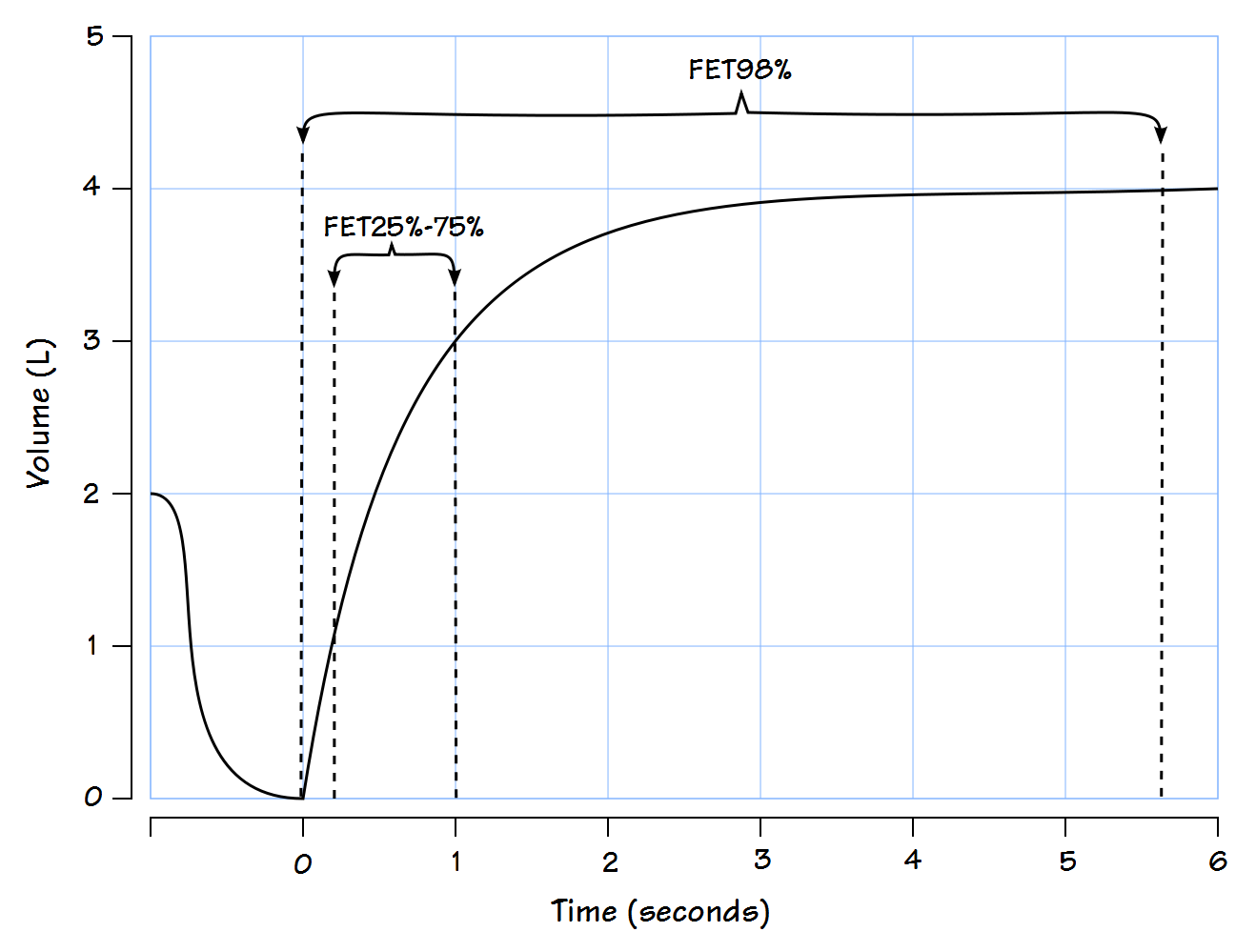
FET25%-75%
The expiratory time between 25% and 75% of the FVC. Also known as the Mid-Expiratory Time (MET), Maximal Mid-Expiratory Flow Time (MMFT) and the Maximal Mid-Expiratory Time (MMET). Although said to correlate well with respiratory resistance there are no reference equations and this measurement never appeared in more than a handful of research articles and textbooks.
FET98%
The expiratory time to 98% of the FVC. Although proposed as a standardized way to measure expiratory time it never saw common use.
There are numerous measurements that can be made from a spirometry maneuver. Simply because a measurement can be made does not mean that it is clinically significant however. In the first decades of modern spirometry many different values were proposed but only a small number of them have survived to the present time. Interestingly, many of the current spirometry systems allow many if not most of these now disused measurements to be reported. About 10 or 15 years ago my lab’s software came bundled with a report format that included almost 20 different values for a single FVC. I’ve seen this report used by at least a couple PFT labs who may have thought that more is better. I’ve also seen some of these measurements used in a variety of research studies, some old, some relatively recent. Their clinical relevance is likely small at best but although these measurements are now mostly gone they have not been completely forgotten.
References:
Hanson JE, Sun X-G, Wasserman K. Discriminating measures and normal values for expiratory obstruction. Chest 2009; 136(6): 369-377.
Ioachimescu OC., Venkateshiah SB, Kavuru MS, McCarthy K, Stoller JK. Estimating FVC from FEV2 and FEV3: Assessment of a surrogate spirometric parameter. Chest 2005; 128(3): 1274-1281.
Knudson RJ, Slatin RC, Lebowitz MD, Burrows B. The maximal expiratory flow-volume curve. Normal standards, variability and effects of age. Amer Rev Respir Dis 1976; 113: 587-600.
Kory, RC, Callahan R, Boren HG, Syner JC. The veterans administration-army cooperative study of pulmonary function I. Clinical spirometry in normal men. Amer J Med 1961; 30(2): 243-258.
Miller WF, Scacci R, Gast LR. Laboratory evaluation of Pulmonary Function, copyright 1987, published by JB Lipincott.
Morris JF, Koski A, Breese JD. Normal values and evaluation of Forced End-Expiratory Flow. Amer Rev Respir Dis 1975; 111(6): 755-762.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License