When Tiffeneau described the FEV1 in 1947 and Gaensler the timed FVC and FEV1/FVC ratio in 1950 this opened up an entirely new territory for pulmonary investigators to explore. Numerous new measurements were rapidly mapped out with often conflicting titles. The situation became confusing enough that the British Thoracic Society met in 1956 specifically to standardize terminology. At this time only the volume-time curve was available for measurement purposes (usually a pen trace on kymograph paper) and this fact helped determine what measurements it was possible for researchers to make.
These measurements were in somewhat common use for the first decades of modern spirometry. They have since mostly passed into disuse and have largely been forgotten either because they were superceded by the flow-volume loop or because they never established any particular clinical value. Even so most of these measurements are included as reporting options in current spirometry testing systems. Despite being of questionable value they are still interesting if for no other reason than that they highlight the incredible number of ways that a volume-time curve can be analyzed.
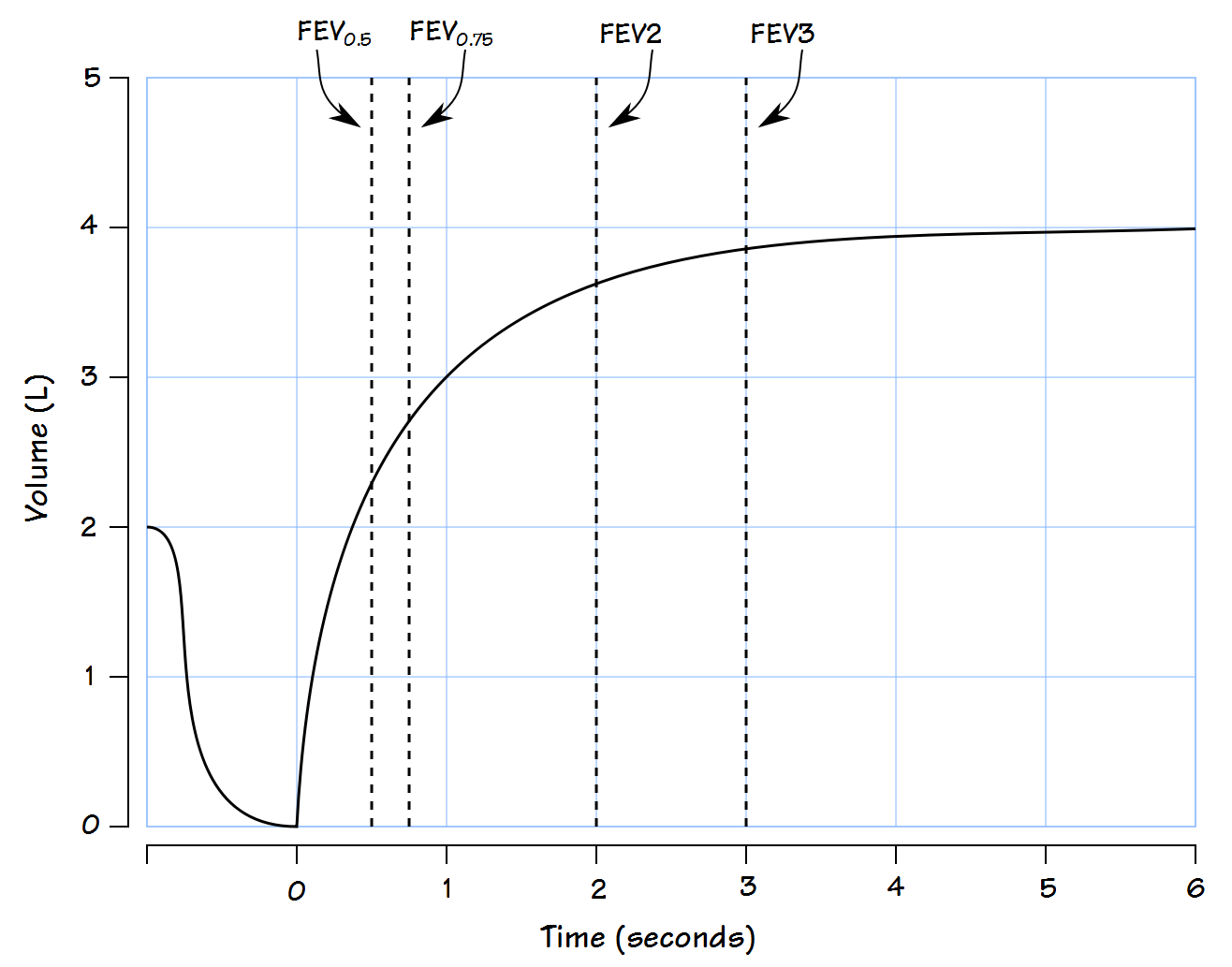
FEV0.5
In retrospect the use of the FEV1 and FEV1/FVC ratio to assess airway function seems inevitable but in the early decades it wasn’t clear what timed measurements were optimal. Like the FEV1 the forced expired volume in 0.5 seconds can be measured from the volume-time curve. The FEV0.5 is considered more reproducible than the Peak Expiratory Flow and has been used to assess cough. Although normal values for the FEV0.5 were included in the reference equations from the 1961 VA-Army and Kunudson’s 1976 spirometry study this measurement has rarely been used in adults but has instead found extensive use when measuring and reporting spirometry in infants and children.