From: Maurice McGregor and Margaret R. Becklake. THE RELATIONSHIP OF OXYGEN COST OF BREATHING TO RESPIRATORY MECHANICAL WORK AND RESPIRATORY FORCE. Volume 40, Issue 6 (June 1961), J Clin Invest. 1961;40(6):971–980.
From Mead J. Volume displacement body plethysmograph for respiratory measurements in human subject. J Appl Physiol 1960; 15:736-740. Article generously provided by Carl O’Donnell, PhD, MPH
From: Mead J. Volume displacement body plethysmograph for respiratory measurements in human subject. J Appl Physiol 1960; 15:736-740. Article provided by Carl O’Donnell, PhD, MPH
From: Woolf CR. An assessment of the Fractional Carbon Monoxide uptake and its relationship to pulmonary diffusing capacity. Chest 1964; 46: 181-189.
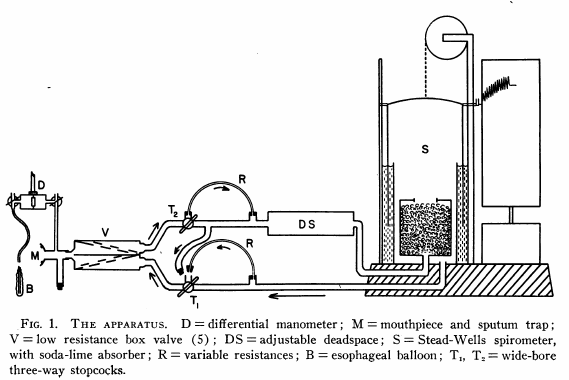
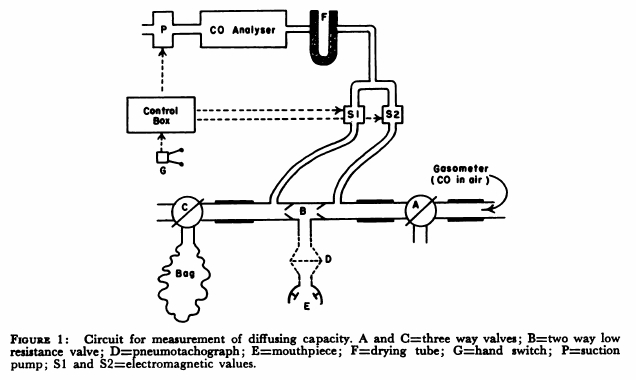
“The technique used to measure diffusing capacity is a modification of the end tidal steady-state method described by Bates. The arrangement of the apparatus is shown in Fig.1. The patient, comfortably seated, breathed through a two-way low resistance valve (B) with the three-way valves (A and C) open to the air. By means of a switch on the control box an electromagnetic valve (S1) was opened and a a small diaphragm suction pump was activated causing expired air to be drawn continuously through a Liston-Becker carbon monoxide analyzer. The reading on the meter of the analyzer gave the correction to be made for expired carbon dioxide. Valve A was turned so that the patient breathed from a recording 350 liter gasometer containing approximately 0.13 per cent carbon monoxide in air. The inspired carbon monoxide concentration was obtained by opening electromagnetic valve S2 and drawing the gas through the analyzer. When a steady reading had been obtained, valve S2 was closed. End tidal gas was obtained by opening valve S1 and activating pump P with a hand switch G during each inspiration. Repeated end-tidal samples were drawn through the gas analyzer until a steady reading for end tidal carbon monoxide concentration was obtained. Then valve C was turned and mixed expired gas collected in a bag for one minute and this completed the test. The mixed expired gas carbon monoxide concentration was obtained by separately passing the bag gas through the carbon monoxide analyzer. Minute volume, respiratory rate and tidal volume were obtained from the recording drum of the gasometer.”
Henderson M, Apthorp GH. Rapid method for estimation of carbon monoxide in blood. Brit Med J 1960: 2: 1853
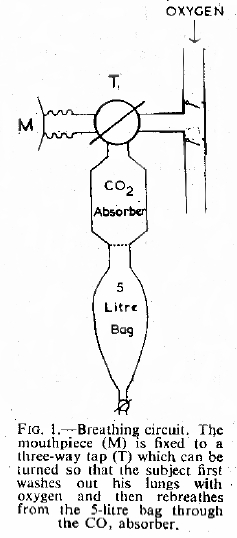
“Each subject washed the nitrogen from his lungs by breathing 100% oxygen from a simple open circuit (Fig. 1) for a period of three minutes. At the end of this time he was instructed to take a maximum inspiration and hold his breath. The three-way tap (T) was then turned and exhaled through a carbon dioxide absorber, previously washed out with oxygen into an empty and rebreathed from this bag for a further three minutes. The contents of the bag were then analysed for oxygen by the Haldane method and for carbon monoxide, using an infra-red meter.”
From Johnson RL, Spicer WE, Bishop JM, Forster RE. Pulmonary capillary blood volume, flow and diffusing capacity during exercise. J Appl Physiol 1960; 15: 893-900
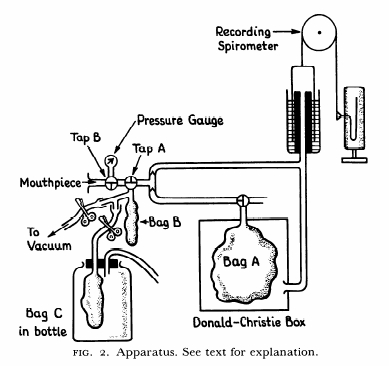
“Measurements were made as follows: after exhaling to residual volume, the subject went on the mouthpiece and rapidly inhaled a measured volume of the gas mixture from bag A. This breath was held for a measured time after which is was exhaled rapidly. The first liter of exhalate was allowed to clear the dead space, after which tap A was turned 90 degrees counter clockwise and an alveolar sample of a bout a liter was collected in bag B. t was not convenient to clamp this wide-mouthed sampling bag and remove it; therefore, the sample was aspirated into another removable bag C, in which it was sealed and set aside for later analysis.”
From Kreuzer F, Van Lookeren Campagne P. “Resting Pulmonary Diffusing Capacity for CO and O2 at Altitude”. J Appl Physiol 1965; 20: 519
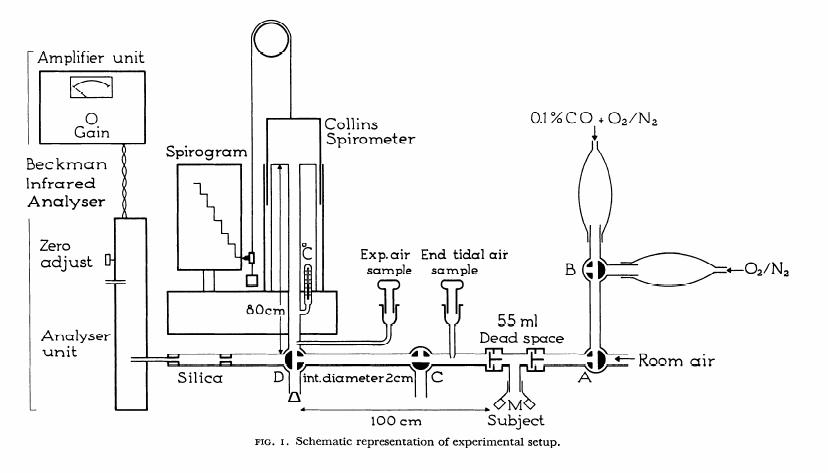
The supine subjects rested for about a half an hour and then breathed, in varying sequence through a low-resistance valve, one of the following gas mixtures listed in Table 1, first without CO for some 10 min, and subsequently with 0.1% CO. In this way similar inspiratory O2 pressures were attained for the three levels of oxygenation at both altitudes (about 80, 150 and 400 mm Hg, respectively, with the following average alveolar PO2 in mm Hg: at sea level 46.5, 1.7.6 and 382; high altitude: 53.6, 117 and 365). After equilibration with the CO-free gas mixture the inspiratory circuit was switched to the corresponding CO-containing muxture (Fig. 1, stopcock A or B). On and one-half minutes were allowed for equilibration with 0.1% CO which is considered sufficient by most authors; aftere simultaneous washing out of spirometer and connections towards the end of this period, stopcocks C and D were turned to collect expired gas in a 9-liter spirometer with continuous recording of breaths during about a a half a minute, bringing total exposure to CO to some min per run.
The diverse, quirky and mostly forgotten history of Pulmonary Function testing