
Over 60 years old and still in use. Collins spirometers are indestructible. Photo courtesy of Gary A. Bulla, Ph.D., Department of Biological Sciences, Eastern Illinois University.
Over 60 years old and still in use. Collins spirometers are indestructible. Photo courtesy of Gary A. Bulla, Ph.D., Department of Biological Sciences, Eastern Illinois University.
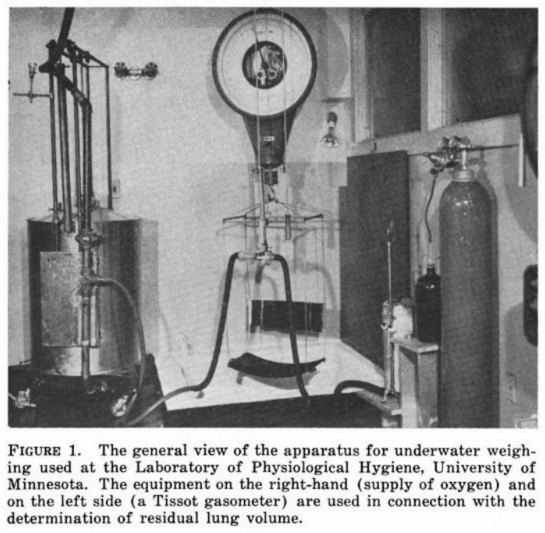
From Techniques for Measuring Body Composition: Proceedings of a Conference, Quartermaster Research and Engineering Center, Natick, Massachusetts, January 22-23, 1959, by Josef Bro_ek, Austin Henschel , published by National Academies, 1961, page 257.

Described as the first spirometer at the Hospital de la Santa Creu i Sant Pau of Barcelona and dated 1958. Manufacturer is unknown but it looks similar to those made by Palmer of England. From a powerpoint presentation for a 2015 Spirometry Course in Barcelona by Felip Burgos from the Hospital Clínic of Barcelona and Jordi Giner from the Hospital de la Santa Creu i Sant Pau of Barcelona, sponsored by Sibelmed.

Described as a Barnes Spirometer manufactured in Poland in the 1950’s. Shown in the un-filled position. Found on an Ebay listing.

Described as a Barnes Spirometer manufactured in Poland in the 1950’s. Showed in the filled position. Found on an Ebay listing.
From Lehrbuch der Stimm und Sprachheilkunde (“Textbook of voice and speech therapy”), Chapter 1, “Die stimm und ihre Storungen” by Prof. Dr. R. Luchsinger, Published by Springer-Verlag, 1959, page 10. Manufacturer was not named.

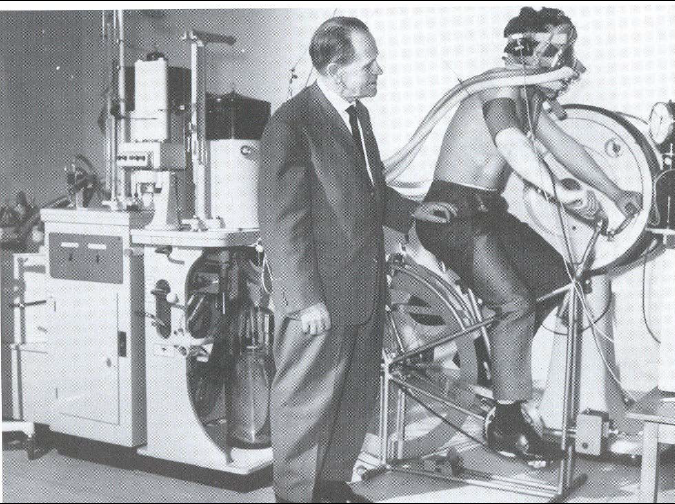
Bicycle ergometry. From: Studien uber die Pathophysiologie der Atmung bei der Silikose Die Lungenfunktion im Arbeitsversuch by P.H. Rossier and A. Buhlmann, 1950, page 58.

Undated photo found on the FAO Corporate Repository. Probably from the 1950’s.
Exercise testing , 1954. Pictured standing is Sepp Herberger, German football coach. Equipment manufacturer was not named but is likely Dargatz. From: page 40 of of a 2003 doctoral dissertion by Yaser Mahfouz Atwa Saad Elgohari.
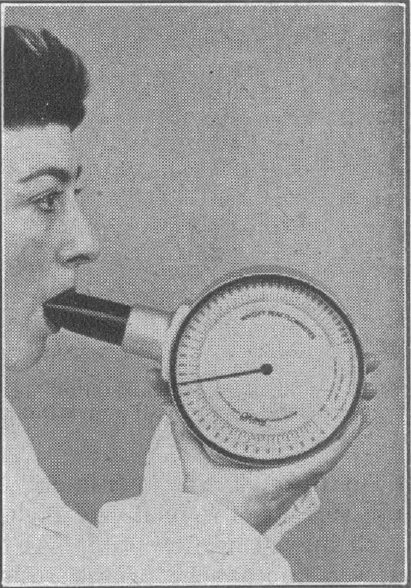
From: Wright, B. M., and C. B. McKerrow. “Maximum forced expiratory flow rate as a measure of ventilatory capacity.” British Medical Journal 1959; 2.5159, page 1043.
“The general appearance of the instrument, which weighs about 2 lb. (900 g.), and its method of use are shown in Fig. 2. The subject is asked to take a deep breath, as for a vital capacity, to place the mouthpiece in his mouth, and then to blow into the instrument as hard as he can. It is not necessary to try and empty the lungs, and it is undesirable to do so, because it is unpleasant and tiring, but a certain amount of “follow through” is required. After a couple of practice blows, three attempts in succession are recorded and the average is taken. This is statistically a more satisfactory procedure than simply taking the highest reading,although logically the latter would be preferable, since a maximum if being measured. Most subjects will give three readings with agree with 10% after the practice tries, but the observer must ensure that the subject is really trying his hardest. As with all ventilatory tests of this kind, including the M.V.V., failure to produce reasonably concordant results usually indicates a lack of co-operation.”