From Traité élémentaire de physique médicale, Wilhelm Max Wundt, Armand Imbert. Published 1884, Paris. A description of its function, from Outlines of Physiology in Its Relations to Man, page 388, by John Gray McKendrick and James Macelhose, 1878 is as follows:
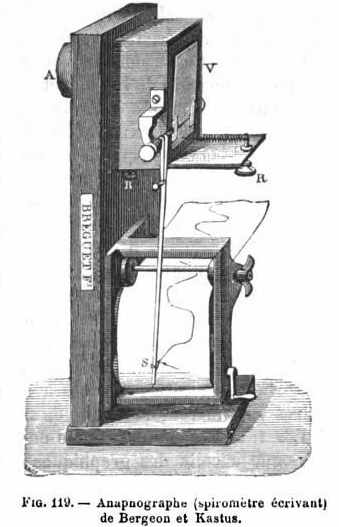
“A valve, or mobile plate of aluminum, V, forms one side of a rectangular box put into communication by A with a respiratory tube terminated by a mouth or nose-piece. The axis of rotation of the valve carries a very light lever, S, which writes on a strip of paper moved by clockwork. If air be propelled through the tube into A with each movement of inspiration and expiration, the variations of the pressure of the air in the air passages are transmitted to the valve which, by the lever, inscribes on the paper. The instrument has been graduated so as to suit bands of paper divided into small squares, each square representing a certain amount of air. Thus the instrument registers not only the pressure of the air, but the quantity inspired and expired, and the rapidity of the current of air. With such instruments, it may be shown that when the lungs have been emptied by as much as possible of air by the most powerful expiratory effort, they still contain a quantity over which we have no control, and which may be estimated at about 100 cubic inches. This has been termed residual air. In addition to this residual air, there are about 100 cubic inches constituting supplemental air, or the air that remains in the chest after an ordinary expiration, in addition to the residual air already mentioned. This there are about 200 cubic inches of air in the lung after a gentle expiration. If then, inspiration takes place gently, from 25 to 30 cubic inches are introduced; these, constituting tidal air, are expelled with the next expiration. We find, therefore, that in ordinary respiration there are 200 cubic inches of air in the lungs, and an inward and outward current of say 30 cubic inches; but, finally, it is possible by a very deep and prolonged inspiration, to introduce 100 cubic inches more. This last quantity is called complemental air. After the deepest inspiration there are, therefore, in the lungs 330 cubic inches of air, which number expresses the maximum capacity of the lung.”