Airway hyper-responsiveness is a primary feature of asthma. There are a number of bronchial challenge tests designed to evoke and measure this factor, the most common of which require the inhalation of one or another bronchoconstrictive agent such as methacholine, histamine, mannitol or hypertonic saline.
An elevated ventilation can cause many asthmatics to bronchoconstrict and this is often the cause of Exercise-Induced Bronchospasm (EIB). There are two competing theories as to why this happens. A number of researchers have suggested that the mechanism is a drying of the airway mucosa which changes the osmolarity of the respiratory tract fluid which in turn causes some cells to releases mediators that cause bronchoconstriction. Other researchers assert that it is the cooling of the airways during hyperventilation and an increased blood flow and edema during subsequent re-warming that causes the bronchoconstriction. There is evidence to support both interpretations and it is likely that both mechanisms coexist, with one or the other being more predominant in any given individual.
Although the inhalation challenge tests are reasonably sensitive not all patients with EIB have a positive reaction. When a patient’s primary complaint is exercise-related or when they have had a negative inhalation challenge test and are still symptomatic, a ventilatory challenge test should be considered. There are several ventilatory challenge tests that are specifically oriented towards evoking and characterizing EIB. These are the Cold Air challenge, Eucapnic Voluntary Hyperventilation and Exercise Challenge. There are a number of similarities between these tests.
Cold Air Challenge
A Cold Air Challenge (CACh) test consists of having a patient hyperventilate while breathing air that has been cooled to a temperature of between -10°C and -20°C. It is usually performed using a mixture of 5% CO2, 21% O2, 74% N2 in order to prevent dizziness from hypocapnia.
Note: some researchers have added carbon dioxide to compressed air rather than using a mixture. Although this lowers the cost of the compressed gases used during the challenge this also requires constant titration of the carbon dioxide flow rate in order to maintain a subject’s PETCO2 at a normal level, which in turn requires an end-tidal CO2 monitor. At least one study showed that 5% CO2 in air maintained a reasonably normal PETCO2 in most subjects across a very wide range of minute ventilations and because this simplifies the testing process a 5% CO2 gas mixture is more commonly used.
The period of hyperventilation is usually 3 to 4 minutes. A number of researchers have used hyperventilation periods of up to 6 minutes but several studies have shown that 3 minutes is usually sufficient to induce bronchoconstriction.
Cold air challenges can be performed with a single level of ventilation or with multiple levels. The advantage of performing a cold air challenge at multiple levels is that it makes it possible to determine what level of ventilation causes bronchoconstriction. When this is done minute targets ventilation are usually 10%, 20%, 40% and 80% of an individual’s observed MVV (or 4, 8, 16 and 32 times the observed FEV1). The disadvantage is that this process can be extraordinarily time consuming. Peak bronchoconstriction usually occurs by 15 minutes post-exposure but more than one investigator has indicated there is a refractory period of up to 60 minutes following exposure. For this reason most cold air challenges are performed with a single level and with a minute ventilation target that ranges from 15 to 30 times the FEV1 or 40% to 80% of measured MVV.
Changes in FEV1, SGaw. SRaw and oscillometry have been used to assess bronchoconstriction following exposure to cold air. FEV1 should be measured at 5 minute intervals up until at least 15 minutes post-exposure. SGaw can be measured as frequently as every 2 minutes post-exposure, but measurements should also continue up to 15 minutes post-exposure. There is no real consensus as to what constitutes a positive response and different researchers have indicated that a positive response for FEV1 is a decrease that ranges from a 9% to 20% and for SGaw it is a decrease that ranges from 30% to 50%. Even though studies performed with presumably normal individuals have shown decreases in FEV1 of up to 10% and SGaw up to 30% the most common guidelines indicate that a 10% decrease in FEV1 and 30% decrease in SGaw should be considered significant. Interestingly, one study indicated that the sensitivity to cold air declined with age but unfortunately this finding has not been confirmed.
Changes in oscillometry values are more difficult to characterize, partly because of differences in equipment (IOS vs FOT) but also in nomenclature. One study using FOT noted increases in resistance at 8 hz and 28 hz, decreases in reactance at 8 hz and an increase in resonant frequency from 12 to 25 hz. Another study using IOS found significant change in R5, X5, X35 and a doubling of the resonant frequency from 12 to 24 hz.
One of the primary technical problems with cold air challenges is providing cold air. Many of the research studies involving cold air used custom-built systems with a variety of refrigeration units and heat exchangers.
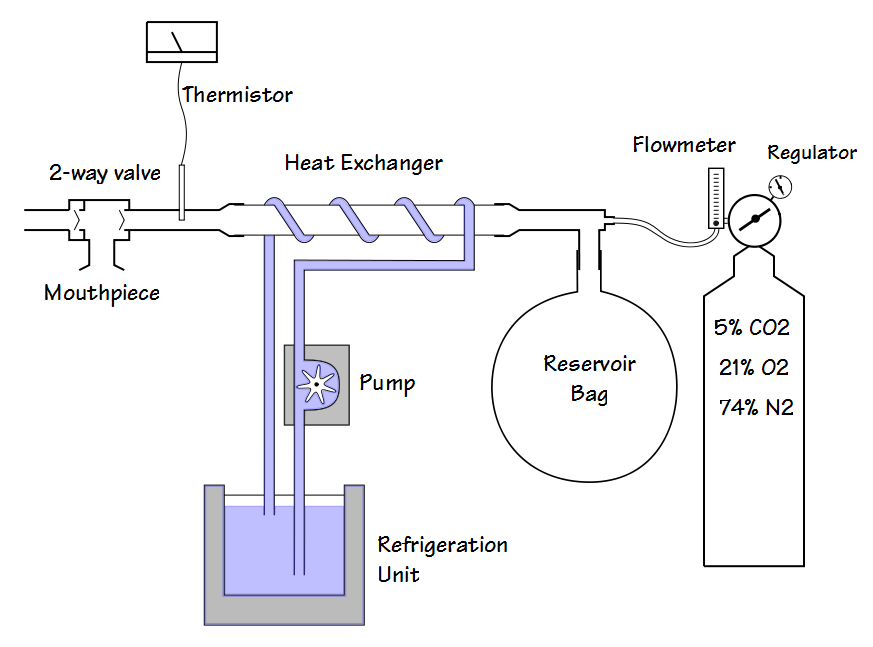
A basic system where the patient’s minute volume is determined by the flow rate of the gas mixture to the reservoir balloon.
At the present time the only cold-air system for medical use appears to be the TurboAire Challenger from Vacumed.
Note: This device is a Ranque-Hilsch vortex tube and is a fascinating application of atmospheric physics.
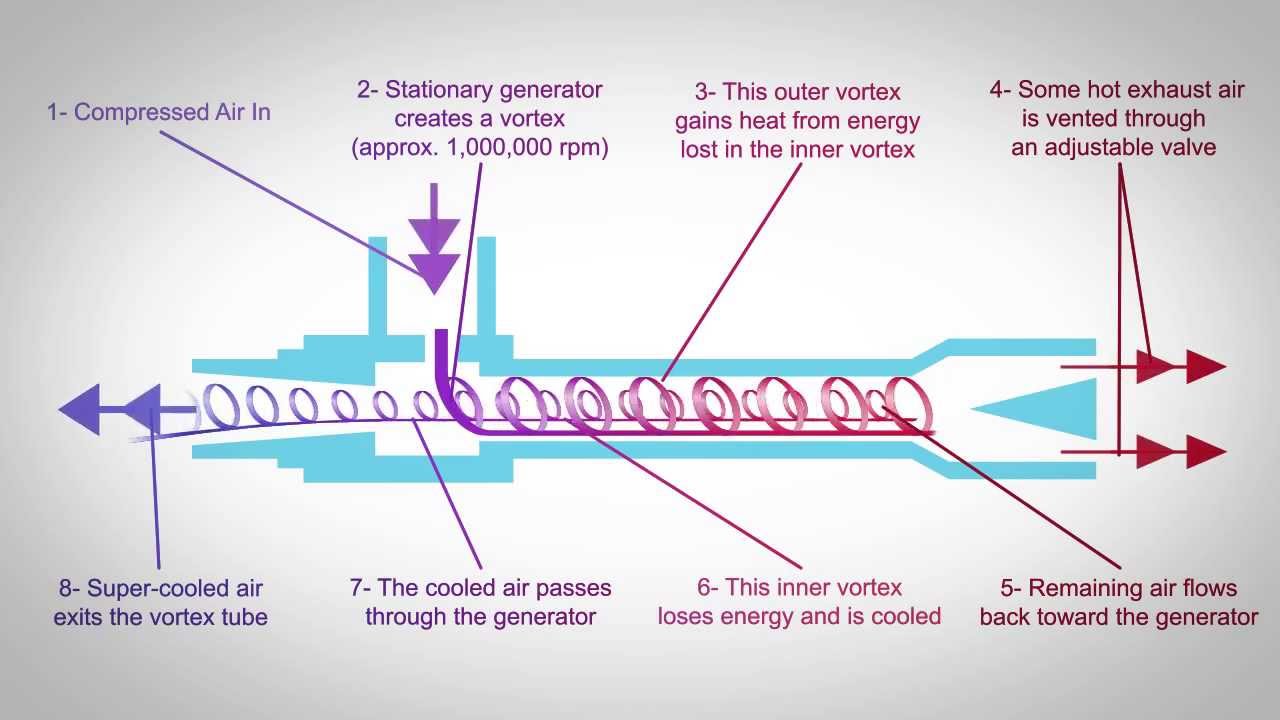
[vortex tube found on youtube, posted by ITW Vortec]
Compressed gas is injected tangentially into a tube. This cause the rapid rotation of air within the tube (up to 1,000,000 RPM!). This in turn causes warm air and cold air to separate and in fact, air loses temperature through a decrease in angular momentum as it acts to increase the radial velocity of the outer layer. Warm air is in the outer layer and exits one end of the tube. Cold air is in the interior of the tube and exits the other end. In one sense this device is inefficient since the majority of the compressed gas is warmed and therefore unusable for testing. On the other hand, there are no moving parts and no bulky refrigeration units or heat exchangers. The TurboAire requires compressed air at 80-110 PSI and flow rates (not published) above what can be provided by hospital wall outlet. For these reasons the source gas will need to be provided by a regulator and gas cylinder.
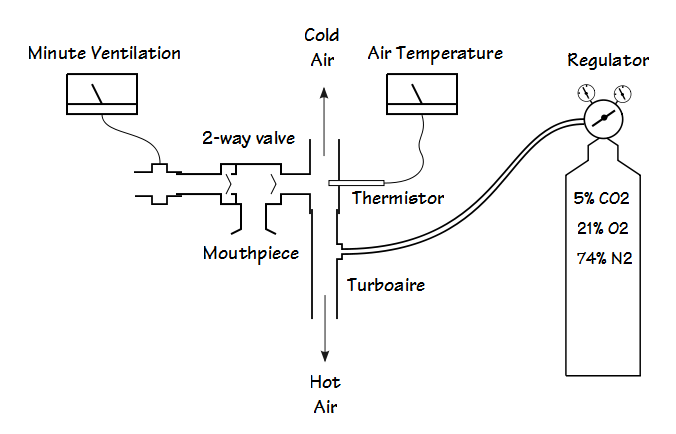
An additional technical problem is monitoring a patient’s minute ventilation during the cold air challenge. Depending on the actual layout of the cold air system this has been done by controlling the flow of gas to a reservoir (Douglas bag), collecting exhaled air in a reservoir and evacuating it at a controlled rate, with an in-line gas meter, or with a flow sensor. Finally, inspiratory temperature should be measured in order to assure the proper gas temperature is being provided.
Eucapnic Voluntary Hyperventilation
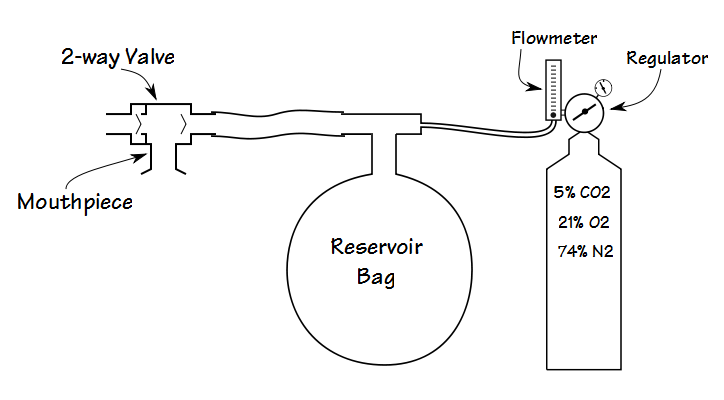
In a real sense, the Eucapnic Voluntary Hyperventilation (EVH) test is a cold air challenge without the cold air, and in fact the EVH was developed after the CACh. Like the CACh subjects breath a mixture of 5% CO2, 21% O2, 74% N2 to prevent hypocapnia. In general there are two different protocols; stepped and single-stage. An example of a stepped EVH would be 3 to 6 minutes of ventilation at:
1) 30% of the MVV
2) 60% of the MVV
3) 90% of the MVV
where MVV is calculated from FEV1 x 35, with spirometry at regular intervals out to 10 minutes following each stage. An example of a single-stage protocol would be 85% of the MVV (FEV1 x 35) for 6 minutes, with spirometry at regular intervals out to 15 minutes.
Although a multiple-step protocol can give some notion as to what constitutes a triggering level of ventilation, at least one study showed that the level of bronchoconstriction, when it occurred, was less than that for a single-step protocol.
One study showed that at decrease in FEV1 greater than 11.3% was outside the 95% confidence limits but other researchers have indicated that a decrease of 10% within 5 to 10 minutes post-hyperventilation should be considered as positive.
The advantage that EVH has over CACh is a simplified testing apparatus without the need to provide cold air. The disadvantage is that it tends to require a higher minute ventilation and for a longer period of time and this may place a limit on which patients can perform it. There is also some evidence that EVH does not evoke as great a bronchoconstrictive response as cold air. One study that compared the two techniques showed a mean decrease in FEV1 of 11.7% with EVH compared to a mean decrease in FEV1 of 20.4% with CACh in the same subjects.
Exercise Challenge
The ATS published standards for exercise challenge testing as part of the standards for methacholine challenge testing. The primary recommendations are the use of a treadmill or bicycle ergometer but field testing, i.e. where the subject exercises outdoors performing the activities that usually lead to their symptoms can also be performed. Since hypocapnia does not occur with exercise the testing is performed with room air. The ATS standards recommended a humidity content less than 10 mg/L but a number of researchers indicate that it should be supplied from a cylinder in order to assure a humidity level of less than 3 mg/L. A number of researchers have combined a CACh with an exercise challenge by providing cold, dry air during exercise.
For safety heart rhythm should be monitored with a 12-lead or 3-lead ECG. The level of exercise is determined by the workload need to either attain a heart rate of 80%-90% of the predicted maximum or to attain a ventilation of 40%-60% of the MVV (FEV1 x 35). In general the exercise workload should progress until the target heart rate or ventilation is achieved and then is maintained at that level for a minimum of 4 minutes. Spirometry is performed at 5, 10, 15, 20 and 30 minutes post-exercise and a positive response is a 10% decrease in FEV1.
Interestingly, although the point is to determine the presence of exercise-induced bronchoconstriction, numerous researchers have shown that an exercise challenge test, which includes field testing, is significantly less sensitive (and less specific) than cold air or eucapnic voluntary hyperventilation challenge tests.
For all of the ventilatory challenge tests most of the same contraindications as for a methacholine or histamine challenge should be applied. Baseline FEV1 should not be less than 65%-75% of predicted and unless their effectiveness is specifically being tested inhaled bronchodilators and steroids should be withheld prior to a challenge. Although severe bronchoconstriction is relatively uncommon it is always a possibility and for this reason the appropriate medications and the ability to summon more advanced aid should always be present.
Given that most of the early cold air systems were custom-built there is likely the perception that performing cold air challenges is difficult and beyond the ability of the average pulmonary function lab. This is not really true since the cost of a TurboAire Challenger is in the same ballpark as many spirometry systems. It also has no moving parts, making it simple to use and maintain.
Note: I have not used the TurboAire Challenger and have no connections with Vacumed, financial or otherwise. I have worked with a cold air challenge system in the past (and repaired it numerous times) but it was custom built using a refrigeration unit that circulated -40°C isopropyl alcohol through a copper heat exchanger.
EVH systems are even simpler however, and can often be built with equipment that a PFT lab may already have on hand so why these are also not more commonly found in pulmonary function labs is unclear.
The Methacholine challenge is probably the most commonly performed test to assess bronchial hyperreactivity. Cold air challenges and Eucapnic Voluntary Hyperventilation are much less commonly performed, and are most often seen in conjunction with sports medicine. Part of the reason for this is that estimates of the prevalence of EIB among athletes range from 11% to as high as 50% depending on the sport, and not surprisingly the higher numbers come from those athletes that are primarily exposed to cold air such as figure skaters and cross-country skiers.
CACh and EVH have been shown to be more specific to EIB than methacholine challenge tests. More than one study has noted that some subjects within their study group responded to methacholine but not cold air and vice versa. Similarly, even for individuals that do respond to both methacholine and cold air there is often a lack of correspondence between the methacholine PC20 and the decrease in FEV1 following cold air. For all these reasons it has been speculated that EIB is actually different from asthma and it would also seem that EIB is best assessed by CACh or EVH.
Addendum:
CPT code 95070: Inhalation bronchial challenge testing (not including necessary pulmonary function tests); with histamine, methacholine, or similar compounds.
CPT code 94070 Bronchospasm provocation evaluation, multiple spirometric determinations as in 94010, with administered agents (eg, antigen[s], cold air, methacholine)
CPT code 94620 Exercise test, simple
References:
American Thoracic Society. Guidelines for Methacholine and Exercise testing – 1999. Amer J Respir Crit Care Med 2000; 161(1): 309-329.
Anderson SD, Argyros GJ, Magnussen H, Holzer K. Provocation by eucapnic voluntary hyperpnoea to identify exercise induced bronchoconstriction. Br J Sports Med 2001; 35: 344-347.
Anderson SD, Brannan JD. Methods for “indirect” challenge tests including exercise, eucapnic voluntary hyperventilation, and hypertonic aerosols. Clin Rev Allergy Immunol 2003; 24: 27-54.
Argyros GJ, Roach JM, Hurwitz KM, Eliasson AH, Phillips YY. The refractory period after eucapnic voluntary hyperventilation challenge and its effect on challenge technique. Chest 1995; 108(2): 419-424.
Aquilana AT. Comparison of airway reactivity induced by histamine, methacholine, and isocapnic hyperventilation in normal and asthmatic subjects. Thorax 1983; 38: 766-770.
Bauer I, Weisner MD. Cold air bronchial provocation. Technical issues and protocol. Copyright 1998, Equilibrated Bio Systems Inc.
Ben-Dov I, Gur I, Bar-Yishay E, Godfrey S. Refractory period following induced asthma: contributions of exercise and isocapnic hyperventilation. Thorax 1983; 38(10): 849-853.
Carlson K-H, Engh G, Mork M, Schroder E. Cold air inhalation and exercise-induced bronchoconstriction in relationship to methacholine bronchial responsiveness: different patterns I asthmatic children and children with other chronic lung diseases. Respiratory Medicine 1998; 92: 308-315.
Eliasson AH, Phillips YY, Rajagopal KR. Sensitivity and specificity of bronchial provocation testing. An evaluation of four techniques in exercise-induced bronchospasm. Chest 1992; 102(2): 347-355.
Evans TM, Rundell KW, Beck KC, Leving AM, Baumanns JM. Airway narrowing measured by spirometry and impulse oscillometry following room temperature and cold temperature exercise. Chest 2005; 128: 2412-2419.
Filuk RB, Serrette C, Anthonisen NR. Comparison of responses to methacholine and cold air in patients suspected of having asthma. Chest 1989; 95: 948-952.
Heaton RW, Henderson AF, Gray BJ, Costello JF. The bronchial response to cold air challenge: evidence for different mechanisms in normal and asthmatic subjects. Thorax 1983; 38: 506-511.
Heaton RW, Henderson AF, Costello JF. Cold air as a bronchial provocation technique. Reproducibility and comparison with histamine and methacholine inhalation. Chest 1984; 86(6): 811-814.
Koskela HO, Rasanen SH, Tukiainen HO. The diagnostic value of cold air hyperventilation in adults with suspected asthma. Respiratory Medicine 1997; 91: 470-478.
Modi M, Eber E, Steinbrugger B, Weinhandl E, Zach MS. Comparing methods for assessing bronchial responsiveness in children: single step cold air challenge, multiple-step cold air challenge, and histamine provocation. Eur Respir J 1995; 8: 1742-1747.
Molphy J, Dickinson J, Hu J, Chester N, Whyte G. Prevalence of bronchoconstriction induced by eucapnic hyperpnoea in recreationally active individuals. J Asthma Early Online, 2013; 1-7.
Nielsen KG, Bisgaard H. Lung function response to cold air challenge in asthmatic and healthy children of 2-5 years of age. Amer J Respir Crit Care Med 2000; 161: 1805-1809.
Porsjberg C, Brannon JD. Alternatives to exercise challenge for the objective assessment of exercise-induced bronchospasm: Eucapnic voluntary hyperpnoea and the osmotic challenge tests. Breathe 2010; 7(1): 53-63.
Randolph C. Diagnostic exercise challenge. Curr Allergy Asthma Res 2011; 11: 482-490.
Roach JM, Hurwitz KM, Argyros GJ, Eliasson AH, Phillips YY. Eucapnic volunetary ventilation as a bronchoprovocation technique. Comparison with methacholine inhalation in asthmatics. Chest 1994; 105(3): 667-672.
Rundell KW, Anderson SD, Spiering BA, Judelson DA. Field exercise vs laboratory eucapnic voluntary hyperventilation to identify airway hyperresponsiveness in elite cold weather athletes. Chest 2004; 125: 909-915.
Scharf SM, Hemier D, Walters M. Bronchial challenge with room temperature isocapnic hyperventilation. Chest 1985; 88: 586-593.
Schmekel N, Smith H-J. The diagnostic capacity of forced oscillation and forced expiratory techniques in identifying asthma by isocapnic hyperpnoea of cold air. Eur Respir J 1997; 10: 2243-2249.
Steinbrugger B, Eber E, Modl M, Weinhandl E, Zach MS. A comparison of a single-step cold-dry air challenge and a routine histamine provocation for the assessment of bronchial responsiveness in children and adolescents. Chest 1995; 108: 741-745.
Wesseling GJ, Vanderhoven-Augustin IML, Wouters EFM. Forced oscillation technique and spirometry in cold air provocation tests. Thorax 1993; 48: 254-259.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License