Since I started performing exercise tests I’ve used both treadmills and bicycle ergometers. There are a several reasons that make ergometers somewhat better for exercise testing than treadmills. Most importantly the reduced noise and physical motion makes it easier to get blood pressure measurements and better quality ECG’s. In addition the workload can be set fairly precisely and they are safer for patients. Treadmills do have some advantages however, since patients are usually able to achieve a higher maximum oxygen consumption (~10%) and for many individuals walking is more natural than riding a bicycle.
When I’ve used a treadmill for exercise testing I’ve always used one version or another of the Bruce protocol. This choice was made by my medical directors but it has always seemed to get patients to their maximum exercise capacity within a reasonable period of time and it seemed to provide reasonable workloads for patients over a broad range of physical abilities. About a dozen years ago (the last time my PFT lab was moved) we no longer had room for a treadmill and replaced it with an ergometer. Since then, I haven’t thought much about treadmills and treadmill protocols.
Recently I was talking with a physician who is going to be performing exercise research with a treadmill. When he showed me the treadmill protocol he was planning on using I thought that the initial speed (3.3 MPH) was too high. Since his study population is going to consist of obese, deconditioned asthmatics, I suggested that for patient safety that it would be better to start at a lower speed and elevation. He asked if I could suggest a different treadmill protocol but I had to reply that all I had ever used was the Bruce protocol.
This brought up an interesting question however, and that is whether there is any such thing as an optimal treadmill protocol. To answer this question I undertook a broad survey of treadmill protocols and have to say that the answer is probably no. Strictly speaking, each treadmill protocol is intended for a specific range of physical effort and the selection of any one protocol has to be based on the expectations and limitations of a patient’s physical abilities.
There are several ways to categorize the different treadmill protocols, but I think that the most relevant may be in their workload. Treadmill workloads are usually expressed in METS. A MET (Metabolic Equivalent of Task) is an oxygen consumption of 3.5 ml/kg/min. The METS that are expected from a given speed and elevation of a treadmill are based on averages and for this reason cannot be used to predict an individual’s actual oxygen consumption.
[Note: Several years ago I got an exercise test report from the hospital’s cardiology lab which included the patient’s maximum oxygen consumption. Since as far as I knew the lab didn’t have a metabolic cart I wondered where the numbers came from. In particular I wondered if they had acquired a metabolic cart and if so why VCO2 and Ve weren’t reported. It turned out the lab had acquired some new stress ECG equipment and the default report included a conversion from the predicted METs of the patient’s treadmill speed and elevation into VO2. They removed this from the report shortly after I asked about it although whether this was due to my question is debatable.]
In particular METS scale poorly with body weight. Nevertheless, METS are a way of gauging the relative workload of different protocols. When looked at in terms of their maximum METS, is is apparent that specific protocols are intended for either debilitated, normal or athletic individuals.
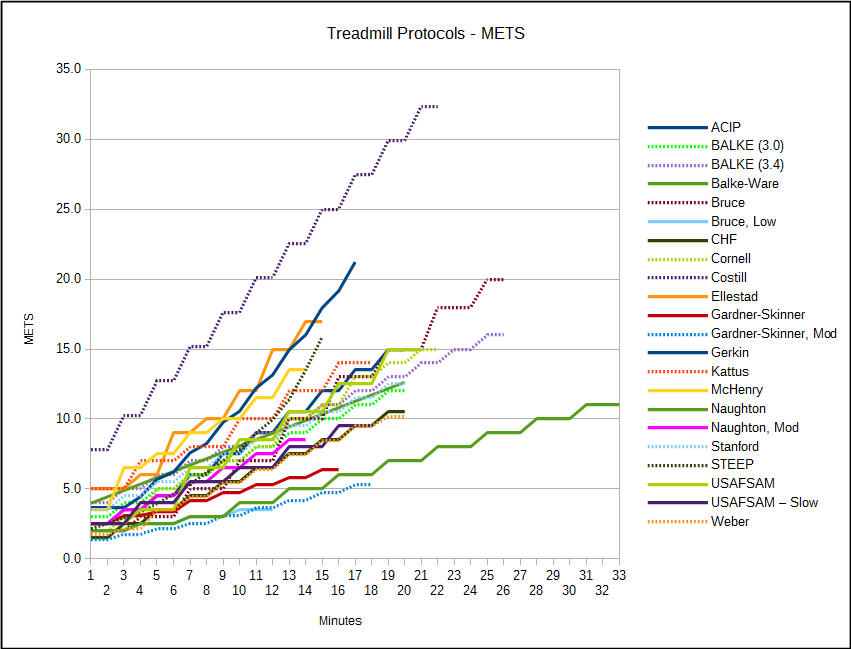
One way to select a treadmill protocol for an individual is therefore by comparing a protocol’s range of METs versus the patient’s expected maximum oxygen consumption. Because METs scale poorly with weight however, the patient’s maximum VO2 in ml/kg/min should probably be obtained from their maximum predicted VO2 in ml/min divided by their predicted body weight rather than their actual body weight. An individual’s maximum expected VO2 needs to be adjusted downwards, of course, if the patient is debilitated and upwards if they are fit and athletic.
Another factor though, is the expected length of the test. There are a variety of reasons to perform exercise tests but my primary reason is to obtain an individual’s maximum oxygen consumption. If an exercise test’s workload increases too fast, the patient’s VO2 may underestimated due to the time constants between oxygen consumption at the cellular level and how it is measured at the mouth. Too steep a workload may also cause an individual to stop the test earlier than necessary simply because the test is “too hard”. On the other hand, if the test’s workload increases too slowly, an individual may stop the test before reaching their maximum VO2 simply because they are exhausted from the length of the test. For maximum VO2 five minutes is likely too short a time period and 15 minutes is probably too long. The optimum length of a test is therefore around 10 minutes and so it is the expected METs at 10 minutes that should be evaluated for a treadmill protocol and not the protocol’s maximum METs.
A final factor when selecting a treadmill protocol has to be patient safety. When an individual has limitations asking them to walk (or run) too fast or to climb too steep of a grade is contraindicated.
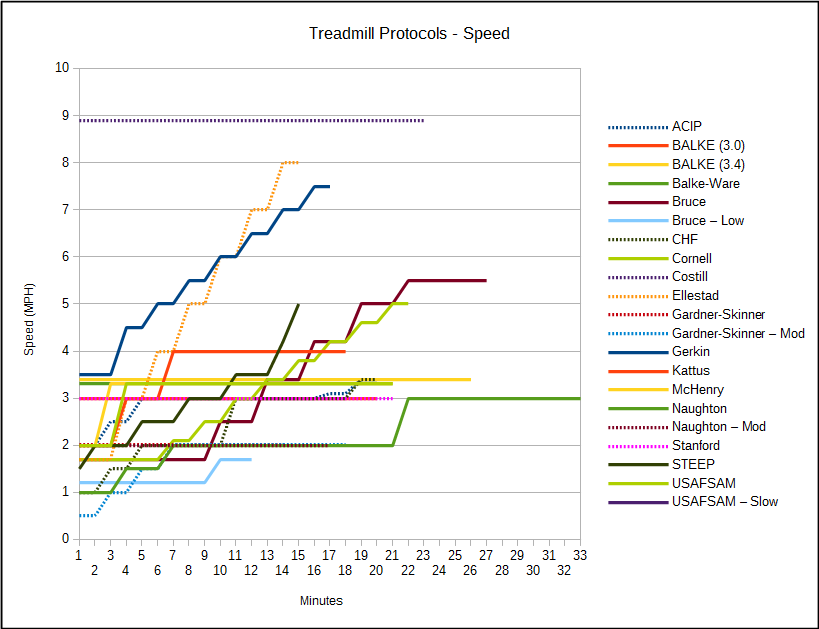
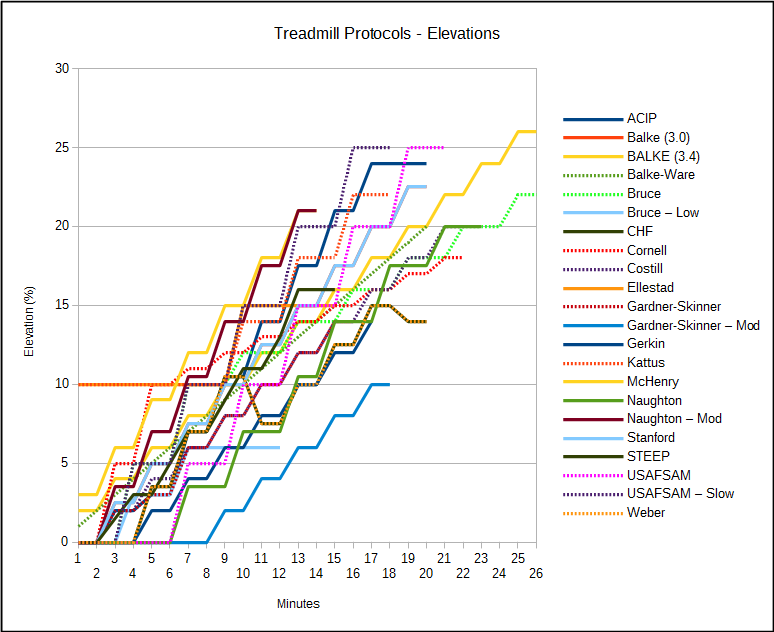
The most commonly used treadmill protocols have fixed changes in speed and elevation. The individual stages are usually specified with a certain time length, but this factor is often modified and the same protocol can have different time lengths. Other than the length of time it takes to get to an individual’s maximum oxygen consumption, I am not sure the length of the stages matters all that much (although if it is too long the test becomes more like a steady state rather than an incremental test). There is a convenience factor in associating changes in speed and/or elevation with blood pressure measurements, but there is no particular reason this has to be the case.
There are a number of treadmill protocols whose speed and/or elevation are not fixed in advance. Several of these allow the patient to set the walking (or running) speed and then just increase the treadmill elevation. There are also a couple that use branching logic and the speed and elevation vary according to values measured during the test. I think that these type of protocols are better suited to a sports medicine setting but there is no reason they can’t be used in a clinical lab.
Once a patient’s expected maximum oxygen consumption, physical status, safety and test length are factored in it is not clear to me that any one treadmill protocol is better than any other. I am used to the Bruce protocol and think that it worked reasonably well at obtaining an individual’s maximum VO2 but at the same time it probably has too steep a workload profile for debilitated patients. For this reason alone any lab that uses a treadmill for exercise testing should be ready to select from at least a couple different protocols based on the patient’s abilities.
Bicycle ergometers are easier because we use a ramp protocol and all we have to do is select rate at which the workload increases. Even though there are reference equations for an individual’s maximum expected workload however, there is still a bit of guesswork involved. Patients often (usually) underestimate or (less frequently) overestimate their abilities but as long as we get a test that is in the neighborhood of ten minutes or so we are usually satisfied. Even so we all have to work with the equipment we have and there is no reason that good quality cardio-pulmonary exercise tests can’t be performed with either an ergometer or a treadmill.
ACIP Protocol, 2-3 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 2.0 | 0 | 2.5 |
| 2 | 2.5 | 2.0 | 3.5 |
| 3 | 3.0 | 3.0 | 4.5 |
| 4 | 3.0 | 7.0 | 6 |
| 5 | 3.0 | 10.5 | 7.5 |
| 6 | 3.0 | 14.0 | 9 |
| 7 | 3.0 | 17.5 | 10.5 |
| 8 | 3.0 | 21.0 | 12 |
| 9 | 3.1 | 24 | 13.5 |
| 10 | 3.4 | 24 | 15 |
Astrand Protocol, modified, subject selects speed, stage 1: 3 minutes, stage 2-7: 2 minutes
| Stage: | Speed (MPH): | Elevation (%): |
| 1 | 5.0 – 8.5 | 0 |
| 2 | 5.0 – 8.5 | 2.5 |
| 3 | 5.0 – 8.5 | 5.0 |
| 4 | 5.0 – 8.5 | 7.5 |
| 5 | 5.0 – 8.5 | 10.0 |
| 6 | 5.0 – 8.5 | 12.5 |
| 7 | 5.0 – 8.5 | 15.0 |
| 8 | 5.0 – 8.5 | 17.5 |
Balke 3.0 Protocol, 2-3 minute stages
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 3.0 | 0 | 3 |
| 2 | 3.0 | 2.5 | 4 |
| 3 | 3.0 | 5.0 | 5 |
| 4 | 3.0 | 7.5 | 6 |
| 5 | 3.0 | 10 | 7 |
| 6 | 3.0 | 12.5 | 8 |
| 7 | 3.0 | 15 | 9 |
| 8 | 3.0 | 17.5 | 10 |
| 9 | 3.0 | 20 | 11 |
| 10 | 3.0 | 22.5 | 12 |
Balke 3.4 Protocol, 2-3 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 3.4 | 2 | 4 |
| 2 | 3.4 | 4 | 5 |
| 3 | 3.4 | 6 | 6 |
| 4 | 3.4 | 8 | 7 |
| 5 | 3.4 | 10 | 8 |
| 6 | 3.4 | 12 | 9 |
| 7 | 3.4 | 14 | 10 |
| 8 | 3.4 | 16 | 11 |
| 9 | 3.4 | 18 | 12 |
| 10 | 3.4 | 20 | 13 |
| 11 | 3.4 | 22 | 14 |
| 12 | 3.4 | 24 | 15 |
| 13 | 3.4 | 26 | 16 |
Balke-Ware Protocol, 1 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 3.3 | 1 | 4.0 |
| 2 | 3.3 | 2 | 4.4 |
| 3 | 3.3 | 3 | 4.9 |
| 4 | 3.3 | 4 | 5.3 |
| 5 | 3.3 | 5 | 5.8 |
| 6 | 3.3 | 6 | 6.3 |
| 7 | 3.3 | 7.0 | 6.7 |
| 8 | 3.3 | 8 | 7.2 |
| 9 | 3.3 | 9 | 7.6 |
| 10 | 3.3 | 10 | 8.1 |
| 11 | 3.3 | 11 | 8.5 |
| 12 | 3.3 | 12 | 9.0 |
| 13 | 3.3 | 13 | 9.4 |
| 14 | 3.3 | 14 | 9.9 |
| 15 | 3.3 | 15 | 10.4 |
| 16 | 3.3 | 16 | 10.8 |
| 17 | 3.3 | 17 | 11.3 |
| 18 | 3.3 | 18 | 11.7 |
| 19 | 3.3 | 19 | 12.2 |
| 20 | 3.3 | 20 | 12.6 |
Bruce Protocol, 3 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 0 | 1.7 | 0 | 2 |
| 0.5 | 1.7 | 5 | 3 |
| 1 | 1.7 | 10 | 5 |
| 2 | 2.5 | 12 | 7 |
| 3 | 3.4 | 14 | 10 |
| 4 | 4.2 | 16 | 13 |
| 5 | 5.0 | 18 | 15 |
| 6 | 5.5 | 20 | 18 |
| 7 | 5.5 | 22 | 20 |
Bruce, Low-Level Protocol, 3 minute stages:
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 1.2 | 0 | 2 |
| 2 | 1.2 | 3 | 2.5 |
| 3 | 1.2 | 6 | 3 |
| 4 | 1.7 | 6 | 3.5 |
CHF (modfied Naughton), 2 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 1.0 | 0 | 1.5 |
| 2 | 1.5 | 0 | 2.5 |
| 3 | 2.0 | 3.5 | 3.5 |
| 4 | 2.0 | 7.0 | 4.5 |
| 5 | 2.0 | 10.5 | 5.5 |
| 6 | 3.0 | 7.5 | 6.5 |
| 7 | 3.0 | 10.0 | 7.5 |
| 8 | 3.0 | 12.5 | 8.5 |
| 9 | 3.0 | 15.0 | 9.5 |
| 10 | 3.4 | 14.0 | 10.5 |
Cornell Protocol, 2 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 0 | 1.7 | 0 | 2 |
| 0.5 | 1.7 | 5 | 3 |
| 1 | 1.7 | 10 | 5 |
| 1.5 | 2.1 | 11 | 6 |
| 2.0 | 2.5 | 12 | 7 |
| 2.5 | 3.0 | 13 | 8 |
| 3.0 | 3.4 | 14 | 10 |
| 3.5 | 3.8 | 15 | 11 |
| 4.0 | 4.2 | 16 | 13 |
| 4.5 | 4.6 | 17 | 14 |
| 5.0 | 5.0 | 18 | 15 |
Costill Protocol, 2 minute stages, can continue past stage 11 as tolerated with 2% increments in elevation.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 8.9 | 0 | 7.8 |
| 2 | 8.9 | 2.0 | 10.3 |
| 3 | 8.9 | 4 | 12.7 |
| 4 | 8.9 | 6 | 15.2 |
| 5 | 8.9 | 8 | 17.6 |
| 6 | 8.9 | 10 | 20.1 |
| 7 | 8.9 | 12 | 22.5 |
| 8 | 8.9 | 14 | 25.0 |
| 9 | 8.9 | 16 | 27.5 |
| 10 | 8.9 | 18 | 29.9 |
| 11 | 8.9 | 20 | 32.4 |
Ellestad Protocol, stage 1: 3 minutes, stage 2-7: 2 minutes.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 1.7 | 10 | 5 |
| 2 | 3.0 | 10 | 6 |
| 3 | 4.0 | 10 | 9 |
| 4 | 5.0 | 10 | 10 |
| 5 | 6.0 | 15 | 12 |
| 6 | 7.0 | 15 | 15 |
| 7 | 8.0 | 15 | 17 |
Gardner-Skinner Protocol, 2 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 2.0 | 0.0 | 2.5 |
| 2 | 2.0 | 2.0 | 3.1 |
| 3 | 2.0 | 3.0 | 3.4 |
| 4 | 2.0 | 6.0 | 4.2 |
| 5 | 2.0 | 8.0 | 4.7 |
| 6 | 2.0 | 10.0 | 5.3 |
| 7 | 2.0 | 12.0 | 5.8 |
| 8 | 2.0 | 14.0 | 6.4 |
Gardner-Skinner modified Protocol, 2 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 0.5 | 0 | 1.4 |
| 2 | 1.0 | 0 | 1.8 |
| 3 | 1.5 | 0 | 2.1 |
| 4 | 2.0 | 0 | 2.5 |
| 5 | 2.0 | 2 | 3.1 |
| 6 | 2.0 | 4 | 3.6 |
| 7 | 2.0 | 6 | 4.2 |
| 8 | 2.0 | 8 | 4.7 |
| 9 | 2.0 | 10 | 5.3 |
Gerkin Protocol, stage 0: 3 minutes, stages 1-14: 1 minute.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 0 | 3.5 | 0 | 3.7 |
| 1 | 4.5 | 0 | 4.4 |
| 2 | 4.5 | 2 | 5.7 |
| 3 | 5 | 2 | 6.2 |
| 4 | 5 | 4 | 7.6 |
| 5 | 5.5 | 4 | 8.2 |
| 6 | 5.5 | 6 | 9.8 |
| 7 | 6 | 6 | 10.6 |
| 8 | 6 | 8 | 12.2 |
| 9 | 6.5 | 8 | 13.1 |
| 10 | 6.5 | 10 | 14.9 |
| 11 | 7 | 10 | 16.0 |
| 12 | 7 | 12 | 17.9 |
| 13 | 7.5 | 12 | 19.2 |
| 14 | 7.5 | 14 | 21.2 |
HALO Protocol, 4 minute stages.
| Stage: | Speed (MPH): | Elevation (%): |
| 0 | Self-paced | 0 |
| 1 | “ | 3.0 |
| 2 | “ | 6 |
| 3 | “ | 9 |
| 4 | “ | 12 |
| 5 | “ | 15 |
| 6 | “ | 18 |
Kattus Protocol, 3 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 2.0 | 10 | 5 |
| 2 | 3.0 | 10 | 7 |
| 3 | 4.0 | 10 | 8 |
| 4 | 4.0 | 14 | 10 |
| 5 | 4.0 | 18 | 12 |
| 6 | 4.0 | 22 | 14 |
McHenry Protocol, 2-3 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 2.0 | 3 | 3.5 |
| 2 | 3.3 | 6 | 6.5 |
| 3 | 3.3 | 9 | 7.5 |
| 4 | 3.3 | 12 | 9 |
| 5 | 3.3 | 15 | 10 |
| 6 | 3.3 | 18 | 11.5 |
| 7 | 3.3 | 21 | 13.5 |
Naughton Protocol, 3 minute stages:
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 1.0 | 0 | 2 |
| 2 | 1.5 | 0 | 2.5 |
| 3 | 2.0 | 3.5 | 3 |
| 4 | 2.0 | 7.0 | 4 |
| 5 | 2.0 | 10.5 | 5 |
| 6 | 2.0 | 14.0 | 6 |
| 7 | 2.0 | 17.5 | 7 |
| 8 | 3.0 | 12.5 | 8 |
| 9 | 3.0 | 15 | 9 |
| 10 | 3.0 | 17.5 | 10 |
| 11 | 3.0 | 20.0 | 11 |
Naughton Protocol, modified, stage 1: 4 minutes, stage 2-7 2 minutes.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 2.0 | 0 | 2.5 |
| 2 | 2.0 | 3.5 | 3.5 |
| 3 | 2.0 | 7.0 | 4.5 |
| 4 | 2.0 | 10.5 | 5.5 |
| 5 | 2.0 | 14.0 | 6.5 |
| 6 | 2.0 | 17.5 | 7.5 |
| 7 | 2.0 | 21.0 | 8.5 |
Stanford Protocol, 2 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 3.0 | 0 | 3.5 |
| 2 | 3.0 | 2.5 | 4.5 |
| 3 | 3.0 | 5.0 | 5.5 |
| 4 | 3.0 | 7.5 | 6.5 |
| 5 | 3.0 | 10.0 | 7.5 |
| 6 | 3.0 | 12.5 | 8.5 |
| 7 | 3.0 | 15.0 | 9.5 |
| 8 | 3.0 | 17.5 | 10.5 |
| 9 | 3.0 | 20.0 | 11.5 |
| 10 | 3.0 | 22.5 | 12.5 |
STEEP Protocol, 1 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 1.5 | 0 | 2.1 |
| 2 | 2 | 0 | 2.5 |
| 3 | 2 | 1.5 | 2.9 |
| 4 | 2 | 3 | 3.4 |
| 5 | 2.5 | 3 | 3.9 |
| 6 | 2.5 | 5 | 4.6 |
| 7 | 2.5 | 7 | 5.3 |
| 8 | 3 | 7 | 6.2 |
| 9 | 3 | 9 | 7.0 |
| 10 | 3 | 11 | 7.8 |
| 11 | 3.5 | 11 | 9.0 |
| 12 | 3.5 | 13 | 10.0 |
| 13 | 3.5 | 16 | 11.4 |
| 14 | 4.2 | 16 | 13.5 |
| 15 | 5 | 16 | 15.9 |
Taylor Protocol, 3 minute stages, 5-10 minute rest periods between stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 3.5 | 10.0 | 8.5 |
| 2 | 7.0 | 0 | 6.4 |
| 3 | 7.0 | 2.5 | 8.8 |
| 4 | 7.0 | 5.0 | 11.2 |
| 5 | 7.0 | 7.5 | 13.6 |
USAFSAM (Modifed Balke-Ware), 3 minute stages:
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 2.0 | 0 | 2.5 |
| 2 | 3.3 | 0 | 3.5 |
| 3 | 3.3 | 5 | 6.5 |
| 4 | 3.3 | 10 | 8.5 |
| 5 | 3.3 | 15 | 10.5 |
| 6 | 3.3 | 20 | 12.5 |
| 7 | 3.3 | 25 | 15 |
USAFSAM – slow, 3 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 2.0 | 0 | 2.5 |
| 2 | 2.0 | 5 | 4 |
| 3 | 2.0 | 10 | 5.5 |
| 4 | 2.0 | 15 | 6.5 |
| 5 | 2.0 | 20 | 8 |
| 6 | 2.0 | 25 | 9.5 |
Weber Protocol, 2 minute stages.
| Stage: | Speed (MPH): | Elevation (%): | METS: |
| 1 | 1.0 | 0 | 1.8 |
| 2 | 1.5 | 0 | 2.1 |
| 3 | 2.0 | 3.5 | 3.5 |
| 4 | 2.0 | 7.0 | 4.5 |
| 5 | 2.0 | 10.5 | 5.4 |
| 6 | 3.0 | 7.5 | 6.4 |
| 7 | 3.0 | 10.0 | 7.4 |
| 8 | 3.0 | 12.5 | 8.5 |
| 9 | 3.0 | 15.0 | 9.5 |
| 10 | 3.4 | 14.0 | 10.2 |
References:
Breithaupt P, Adamo KB, Colley RC. The HALO submaximal treadmill protocol to measure cardiorespiratory fitness in obese children and youth: a proof of principle study. Appl Physiol Nutr Metab 2012; 37: 308-314.
Evans CH, White RD editors. Exercise testing for primary care and sports medicine physicians. Published by Springer, 2009
Froelicher VF, Brammell H, Davis G, Noguera I, Stewart A, Lancaster MC. A comparison of the reproducibility and physiologic response to three maximal treadmill exercise protocols. Chest 1974; 65(5): 512-517.
Froelicher VF, Thompson AJ, Davis G, Triebwasser JH. Prediction of maximal oxygen consumption. Comparison of the Bruse and Balke treadmill protocols. Chest 1975; 68(3): 331-336.
Northridge DB, Grant S, Ford I, Christie J, McLenachan J, Connelly D, McMurray J, Ray S, Hnderson E, Dargie HJ. Novel exercise protocol suitable for use on a treadmilll or bicycle ergometer. Br Heart J 1990; 64: 313-316.
Smokler PE, MacAlpin RN, Alvaro A, Kattus AA. Reproducibility of a multi-stage near maximal treadmill test for exercise tolerance in angina pectoris. Circ 1973; 48: 346-351.
Swank AM, Serapiglia L, Funk D, Adams KJ, Durham M, Berning. Development of a branching submaximal treadmill test for predictive VO2 max. J Strength and Conditioning Res 2001; 15(3): 302-308.
Tierney MT, Lenar D, Stanforth PR, Craig JN, Farrar RP. Prediction of aerobic capacity in firefighters using submaximal treadmill and stairmill protocols. J Strength Conditioning Research 2010; 24(3): 757-764.
White RD, Evans CH. Performing the exercise test. Primary Care 2001; 28(1): 29-53.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
Hello .
First very much thanks for this review, is very much useful and clear. I have a little question ,ERS has published Use of exercise testing in the evaluation of interventional efficacy: an official ERS statement and there they cited the paper of Porszasz J, Casaburi R, Somfay A, et al. A treadmill ramp protocol using simultaneous changes in speed and grade. Med Sci Sports Exerc 2003; 35: 1596–160, do you have any experience with this ecuation.
thanks
Alejandro –
Thank you for the reference. I had not run across this protocol before and have not used it. Reading the article I can see it’s specifically designed to provide a linear increase in work rate and is individualized (i.e the rate at which the treadmill speed and slope advance) based primarily on patient weight. I would have thought that patient height should also have been a factor but given the way they described the math for the work rate that may not be necessary and the results seem to bear that out. The linearity would probably have some advantages when analyzing CPET results. The fact that it is designed to reach a subject’s maximum workload in 10 minutes also places a reasonable limit on the exercise time. They used a standard Sensormedics treadmill but I did not see an explanation of how it was controlled to follow the individualized protocols and that may make it a bit more difficult to implement.
Regards, Richard
hi, thanks for this article,,,,,i am very happy to know the many protocol in the treadmill training.
Which Mets formula did you use?
Mirko –
I never found a particularly good use for METS other than comparing theoretical treadmill workloads and even the assumption it can be used for that is flawed. Actual VO2 depends not just on treadmill speed and elevation but on a subject’s height, stride length, weight, gender and age.
– Richard
Good morning. It’s nice to meet you.
First of all, I am very grateful for the excellent materials and the great contents.
I am a physical therapist who works mainly for stroke patients.
I have some questions and would like to hear your opinion as an expert.
Are there appropriate protocols for performing treadmill exercise stress tests for stroke patients?
I am watching the Webber protocol for two minutes. Are there any papers or facts that can be referred to in more detail?
I believe that your answer will be a cornerstone of great help for stroke patients who are struggling in other countries. Thank you.
Se Kwang Yeo –
Each patient will have individual needs based on the location and severity of the stroke and I speak from experience because my wife is a stroke survivor I’ve been to many therapy sessions with her. A treadmill will only be appropriate for patients that retain sufficient bilateral strength and mobility in their legs to walk without assistance but since since full or partial arm paralysis is relatively common they would have limited ability to grip the side rails and I would still be concerned about their safety. Any patient with a left- or right-sided deficit that requires a cane or a walker or even just affects their gait will find it a struggle to walk on a treadmill, and again safety is an issue. My basic recommendation would be that the treadmill you use with stroke survivors should have a safety harness (something like the ones used for parachutes) tethered above the treadmill so that if a patient does trip or tumble they don’t fall more than a couple of inches. This makes any treadmill testing safe for them and should give the patients the confidence to exert themselves more than they would otherwise. A specific treadmill speed and elevation protocol doesn’t matter all that much since the ability of each patient will differ greatly based on their age, gender and stroke location. Start with a speed and elevation that’s well within their ability and just increase both in small increments. Make sure you test the safety harness on yourself, however, at different speeds and elevations before trying it on any patients. This will help you learn the right way to adjust the both the harness and the height of the tether, and will give you confidence to use it on your patients.
Regards, Richard
Thank you very much for your kind and detailed reply.
First of all, I hope your wife and family are healthy.
I have a dream to carry out a lot of studies on exercise tests and exercise interventions for stroke patients in the future.
Your answers will help me and my research team.
I hope that thanksgiving and joy will be filled with planning. Thank you.
Hi-
Could you please provide me with the reference you used to determine MET’s? Some of the Modified Naughton MET’s you have listed are slightly off
Debbie –
I found the METS for the Naughton protocol on a webpage (https://ssas.com/disability-medical-tests/cardiovascular/treadmill-stress-testing/protocols/) however that website no longer appears to exist. The article did not list any specific references for any of the treadmill protocols it had listed. The METS for the Bruce and Balke protocols on that webpage matched other sources so I had no reason to believe there was any problem with the Naughton protocol.
Regards, Richard