I used to think that spirometry and diffusion capacity tests were hard and that lung volumes were easy. That may have been true in terms of getting patients to do the tests but I’ve long since come to the conclusion that it is easier to assess the quality of spirometry and diffusing capacity tests and know whether you have reasonably accurate results than it is to do this for lung volumes regardless of which lung volume measurement technique you use.
I was reviewing a set of plethysmographic lung volume tests when I noticed something very odd about the reported results. I usually look at just the VTG loops and the volume-time graphs in order to assess test quality. The testing software automatically selects and averages all VTG efforts and when I reviewed them there were a couple loops that were poor quality and I manually de-selected them. I was reviewing this report because the reported lung volume results didn’t quite match what the spirometry results were saying so this time I also took a close look at the numbers after I removed the low-quality loops. That’s when I realized that the reported TLC was larger than the two tests it was averaged from.
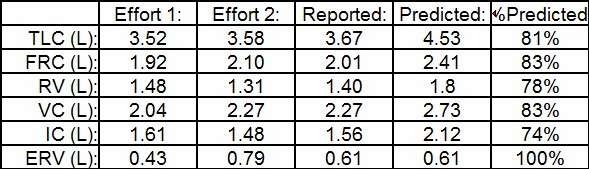
This actually made a difference in how the test results would be interpreted. The largest TLC of the two test efforts was 79% of predicted, slightly below the 80% cutoff we use for the normal range. The averaged TLC was 81% of predicted, slightly above the cutoff, so although it was suspiciously low, it was WNL.
How did this happen?
A close look at the numbers showed me that when the software averages two (or more) different tests, it averages the FRC and ERV but then uses the largest VC. This is completely in line with the ATS-ERS recommendations but also highlights one of the problems in interpreting results.
From: ATS/ERS Standardisation of Lung Function Testing: Standardisation of the measurement of lung volumes. Eur Respir J 2005; 26: page 512
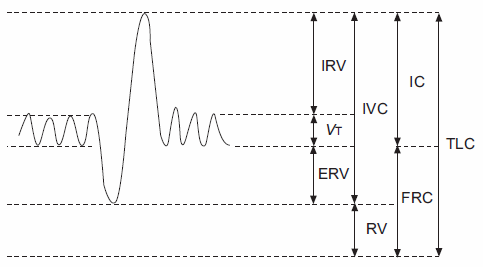
All lung volume tests, regardless of technique, actually measure FRC, the volume in the lungs after an unforced exhalation. A slow vital capacity test (SVC) is performed either immediately before or immediately after the FRC measurement. When the SVC results are compared to the location of FRC it is then possible to determine the Inspiratory Capacity (IC) and the Expiratory Reserve Volume (ERV). Lung volumes are then derived from:
RV = FRC – ERV
TLC = RV + VC
FRC volume is the result of the balance of forces between the lung and the rib cage. It can be affected by an individual’s breathing pattern and tends to vary slightly over time. This is normal and strictly speaking changes in FRC should not affect TLC or RV, but will instead primarily affect IC and ERV.
The first and second lung volume test efforts had mostly similar results. The FRC was only 0.18 L different, the TLC was only 0.06 L and the RV were only 0.17 L different, all of which are well within the guidelines for reproducibility. The biggest difference was between the SVC and ERV results which were 0.23 L and 0.36 L different, respectively.
Although this averaging process follows the ATS/ERS recommendations is this really the correct way to calculate TLC? I understand that because FRC can vary from test effort to test effort that it makes sense to average FRC results and that because IC and ERV are affected by changes in FRC is also makes sense to average them. I also understand that the largest SVC, since it is presumably the most accurate reflection of the patient’s vital capacity, should be used. What this overlooks is that ERV is as much affected by the quality of the SVC as it is by the FRC.
My general experience is that patients can usually perform the IC port of the SVC maneuver correctly almost every time. ERV on the other hand is the effort-dependent part of the SVC and depends on how much the patient is willing or able to push themselves. In this case a not-so-good ERV from the first effort was averaged with a significantly better ERV from the second effort. This blunted the quality of the reported ERV measurement and then when the largest SVC effort was added to it, it actually produced a higher reported TLC than in the test efforts it was averaged from.
I think that since RV is the amount of air left in the lung after a maximal exhalation the lowest value measured in any lung volume test effort could be considered the most accurate value. If this premise is accepted then when lung volume tests are averaged the lowest value of RV and the highest value of SVC should be used to calculate TLC. If this approach was taken, then for this example at least there wouldn’t have been a significant difference between test efforts and reported results. That doesn’t make it the correct approach, however.
The accuracy of any single lung volume measurement test is always suspect. This is why reproducibility is so important and why test efforts are averaged. The reported TLC is affected not only by the quality of the FRC and SVC measurements but also by the quality of the ERV measurement. Different assumptions in the averaging process will produce different TLC and RV measurements from the same set of test efforts. The problem is that assumptions are just that, assumptions.
At the moment I have no evidence that using the lowest RV rather than averaging ERV results leads to a more accurate TLC and in most instances this probably wouldn’t make a significant clinical difference. In this particular case however, the minor differences in TLC straddled the normal cutoff and it does make a difference.
Are you beginning to see why I think that spirometry and DLCO tests are usually easy in comparison?
References:
Brusasco V, Crapo R, Viegi G. ATS/ERS Standardisation of Lung Function Testing: Standardisation of the measurement of lung volumes. Eur Respir J 2005; 26: 511-522.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Dear Sir
I’m having a problem to understand IOS result such as ; CO5 and CO10. What were CO stand for
Thank you
Mangsor –
IOS data is usually presented as Xrs (reactance) and Rrs (resistance). My only guess is that CO is conductance (usually reported as Grs) which is the inverse of resistance.
Regards, Richard