Last week I was reviewing the exercise test results from a patient that appeared to have a relatively straightforward cardiovascular limitation when I noticed the patient also had severe anemia (Hgb = 7.1). Once that fact came up it was no longer clear the patient actually had a cardiac limitation at all.
First the results:
| Rest: | %Predicted: | AT: | %Predicted: | Max: | %Predicted: | |
| VO2 (LPM): | 0.33 | 13% | 0.73 | 28% | 1.45 | 56% |
| VO2 (ml/kg/min): | 5.0 | 11.0 | 21.6 | |||
| VCO2 (LPM) | 0.26 | 0.63 | 1.81 | |||
| RER: | 0.73 | 0.83 | 1.24 | |||
| SaO2: | 98% | 97% | 97% | |||
| PetCO2: | 35.2 | 38.6 | 31.8 | |||
| Ve/VO2: | 34 | 26 | 43 | |||
| Ve/VCO2: | 47 | 31 | 35 | |||
| Ve (LPM): | 11.6 | 8% | 19.2 | 13% | 62.9 | 44% |
| Vt (L): | 0.78 | 1.29 | 2.19 | |||
| RR: | 15 | 15 | 29 | |||
| HR (BPM): | 61 | 35% | 92 | 52% | 152 | 85% |
| BP (mmHg): | 92/62 | 102/64 | ||||
| O2 Pulse (ml/beat): | 5.8 | 39% | 8.2 | 55% | 9.8 | 66% |
Other values calculated from the data include:
| Ve-VCO2 (rest to AT): | 23.8 |
| Ve-VCO2 (rest to peak): | 31.6 |
| Chronotropic Index: | 1.54 |
The maximum VO2 of 1.45 LPM (56% of predicted) indicates a moderate reduction in exercise capacity but overall the patient gave a good exercise test effort and this shown by the elevated RER at peak exercise (1.24) and the maximum heart rate (85% of predicted).
The test results show a cardiovascular limitation fairly clearly. This is in part because any significant pulmonary limitations are ruled out by:
- Normal SaO2 throughout exercise
- Maximum Ve was 44% of predicted
- Ve/VCO2 at AT <35 and Ve-VCO2 slope (rest to AT) <34.
On the other hand, the typical features of a cardiovascular limitation are present:
- Low VO2 at AT (28% of predicted)
- Low maximum O2 pulse (66% of predicted)
- Elevated Chronotropic Index (1.54)
These kind of results are usually the result of a low cardiac output. Specifically, anaerobic threshold will occur early when the heart is unable to deliver enough oxygen to the exercising muscles. O2 pulse is a product of stroke volume and the A-v O2 content difference and when SaO2 is normal, it is a reasonable (although certainly not exact) index of stroke volume so a reduced O2 pulse suggests that the stroke volume is also reduced. Something similar is being said by the chronotropic index, since an elevated value (above 1.30) says that heart rate is advancing faster than oxygen consumption which would also be expected if the stroke volume is low.
But all of this assumes that the amount of oxygen being carried by the blood is reasonably normal and this is not true when anemia is present. Remember the O2 content of blood is determined by:
(Hgb x 1.36 x SaO2) + (0.0031 x PaO2)
So the amount of oxygen that can be carried by the blood is directly related to the hemoglobin concentration:
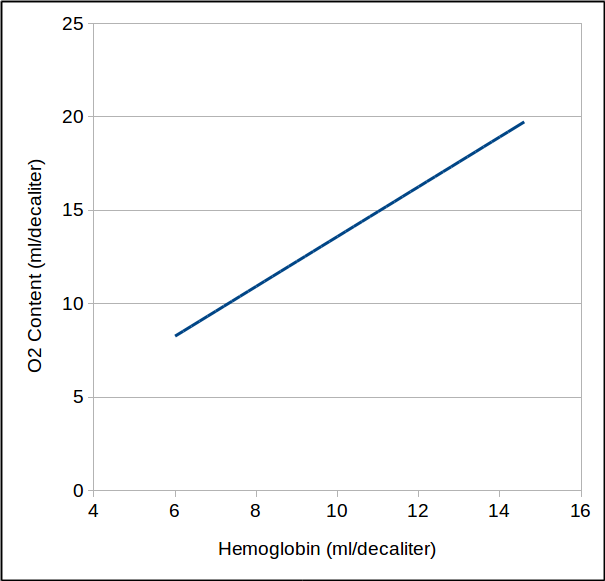
Strictly speaking therefore, when hemoglobin is 7.1, blood can only carry about 9.7 ml/decaliter of oxygen which is slightly less than half it could carry if the hemoglobin was normal (19.7 ml/decaliter), which in turn means that the heart has to pump twice as much blood to deliver the same amount of oxygen.
So did this patient really have a cardiovascular limitation? Probably not, or at the very least, probably not nearly as much of one as these results would usually seem to indicate. The only way to be sure however, would be to repeat the test after the patient’s hemoglobin has returned to normal.
I usually try to find recent hemoglobin results for our CPET patients, just as I would for DLCO patients. Our criteria however, is that a hemoglobin measurement needs to have been made within the last month to be relevant. This is admittedly arbitrary but neither the 2005 nor the 2017 ATS/ERS standards for DLCO testing state how recent a hemoglobin needs to be in order to be used for correction. Although hemoglobin measurements aren’t all that uncommon the fact that it needs to be recent means when it comes to either a CPET or a DLCO most of our patients don’t have one that we can use.
The ability of hemoglobin to carry oxygen is a basic part of physiology. We’re all reasonably aware of the need to correct DLCO tests for hemoglobin but despite this anemia is an often overlooked factor in exercise tests. Because anemia lowers the oxygen carrying capacity of the blood it can mimic or exacerbate a cardiovascular limitation and this needs to be kept in mind when interpreting CPET results.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
If we’re getting an ABG during exercise we’ll request a Hg on the sample for the same reason. For DLCO if no recent Hg then we’ll obtain a pulse co-oximetry reading and then use that value to suggest that ordering physician correlate it against a lab obtained value.
Very nice sharing, really informative and helpful about anemia