Last week I ran across a couple errors in some DLCO tests that I don’t remember seeing before, or at least not as distinctly as they appeared this time. If I hadn’t been looking carefully I could have missed them but both sets of errors will be a lot more evident when the 2017 ERS/ATS DLCO standards are implemented.
The first error has to do with gas analyzer offsets. What alerted me was a set of irreproducible DLCO results.
| Test 1: | Test 2: | Test 3: | Test 4: | |
| DLCO (ml/min/mmHg): | 24.53 | 17.21 | 12.91 | 6.74 |
| Inspired Volume: | 1.99 | 2.06 | 2.32 | 2.26 |
| VA (L): | 3.83 | 3.52 | 3.63 | 2.60 |
| Exhaled CH4: | 43.27 | 49.19 | 54.80 | 74.14 |
| Exhaled CO: | 16.09 | 23.15 | 31.39 | 49.46 |
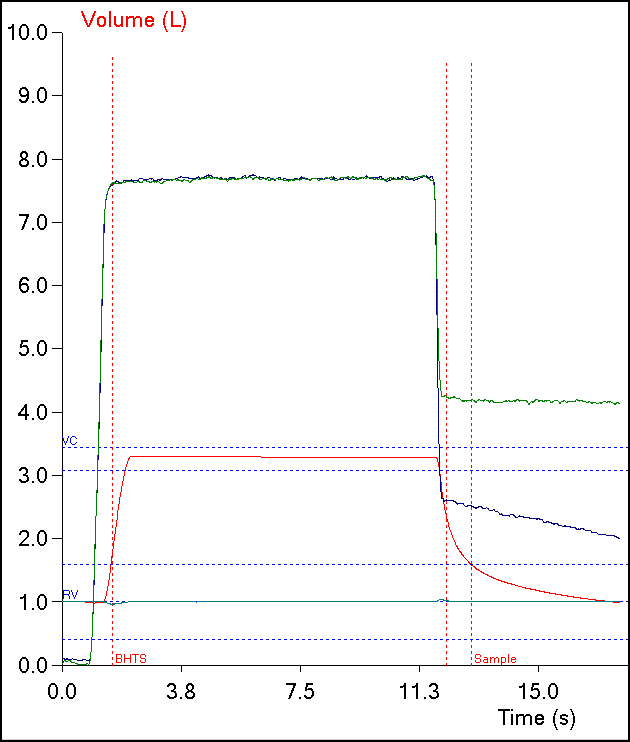
When I first looked at the graphs for each test, there wasn’t anything particularly evident until I pulled up the graph for the fourth DLCO test:
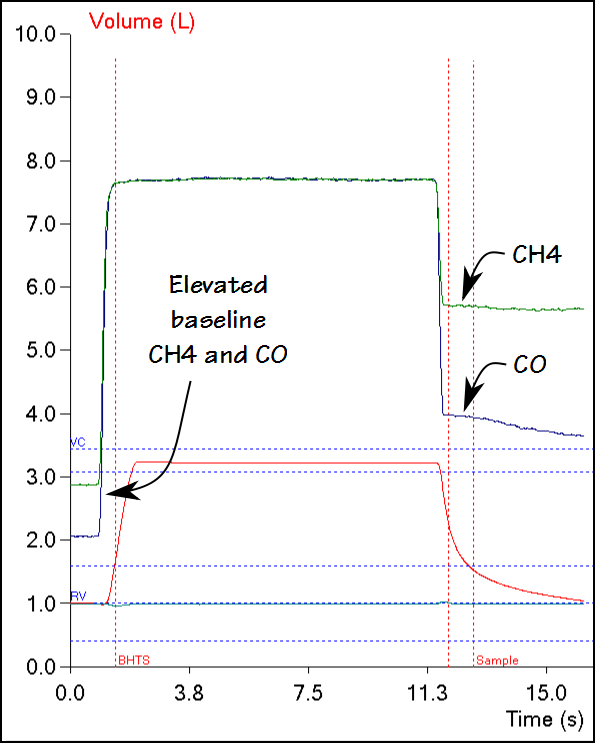
This graph showed that the baseline CH4 and CO readings were significantly elevated, but this hadn’t been evident in the previous tests.