Recently I was reviewing test results from another PFT Lab that uses equipment from a different manufacturer than what my lab uses. When I came to the lung volumes it became evident that the FVC had been substituted for the SVC. I understand the point of using the largest vital capacity when calculating TLC and RV but there are some issues affecting these values when this is done.
Strictly speaking using the FVC is permitted by the ATS/ERS guidelines on lung volume testing, but how an FVC is to be used, as opposed to an SVC, is not addressed. The reason this is an issue is that all lung volume tests regardless of which method is used do not measure TLC and RV directly, they measure FRC. The preferred ATS/ERS TLC calculation is then:
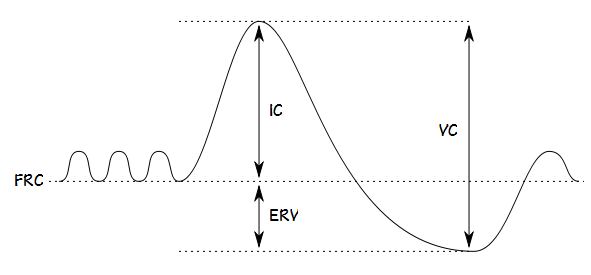
RV = FRC – ERV and TLC = RV + VC
But
TLC = FRC + IC and RV = TLC – VC
is also permitted.
IC and ERV are not explicitly measured from an FVC maneuver and are instead measured during an SVC measurement.
It is here is where the problems of using an FVC in lung volume calculations appears. Specifically, the FVC was substituted for the SVC because the SVC was smaller than the FVC. When this happens then either the IC or the ERV (or both) are also smaller than they “should” be but there is no way to tell which of these is the case. My general inclination is to believe the ERV is reduced since exhaling to RV is harder than inhaling to TLC but I’ve run across many instances where the opposite occurred.
Further inspection of the reported lung volumes showed another problem, however. It was evident that the system was calculating TLC from IC + FRC and then RV from TLC – VC. When this order of calculations is performed the ATS/ERS lung volume guidelines state that “The TLC is the mean of the three largest sums of technically acceptable FRC values and linked IC maneuvers.” The system was averaging the FRC measurements but instead of averaging FRC + IC it was selecting the largest IC from all of the SVC measurements that had been made. This means that the reported TLC was calculated from (mean FRC) + largest IC.
Note: If the calculation started with RV = FRC – ERV the ATS/ERS statements explicitly say that both the FRC and ERV are to be averaged.
The largest IC may or may not be the correct value to use. FRC is a dynamic value and changes as compliance, posture, ventilation and muscle tone change. FRC, IC and ERV can undergo noticeable changes without there being any change in TLC and RV. This is the reason that the ATS/ERS guidelines emphasize “linked” maneuvers. It is true that the largest IC could be a reflection of the best quality SVC maneuver but there is no guarantee this is the case.
Strictly speaking the actual difference between the FVC and SVC was less than 0.2 liter. The TLC and RV calculated using the FVC rather than the SVC are therefore likely near what they would have been with a more optimal SVC. The problem is that because the VC, IC and ERV came from different maneuvers there is no way to say whether the TLC and RV were accurate, overestimated or underestimated.
An additional concern with these lung volumes is that none of the staff from the PFT Lab where the lung volume tests were performed were aware that the test system software was automatically substituting FVC for SVC. Since the SVC was not present on the report the only way to determine how different it was from the FVC was to review the raw test data.
Neither was anyone aware that the largest IC was being added to the average FRC to calculate TLC but this was also not evident on the report and it took me a fair amount of digging in the raw test data to determine this was happening. These facts may well be in the test system’s manual but this was not evident from a quick review.
There is no particularly good answer to this problem. There are good reasons to use the largest VC, both when calculating the FEV1/VC ratio and when calculating lung volumes. Other than stating that it is acceptable to use an FVC in lung volume measurements however, the ATS/ERS guidelines do not address how to use an FVC and instead speak only of linked FRC, IC and ERV measurements. Because of this limitation in the ATS/ERS guideline individual manufacturers are left to decide for themselves whether or not a larger FVC should be substituted for a smaller SVC, and then to decide how to properly calculate TLC and RV.
When a manufacturer claims to meet ATS standards users however, have every reason to expect that calculations are performed accurately and that a minute inspection of the calculation algorithms is unnecessary. In this case the manufacturer can accurately claim that they are meeting the ATS/ERS guidelines when they substitute FVC for SVC although I would point out that using the largest IC is not an appropriate interpretation of the guidelines.
My preference would be that because using FVC instead of SVC has the potential to introduce more error into the calculation of TLC and RV it should not be used. I am biased however, because I am used to judging lung volume test quality based on the “real” SVC and find this more difficult when a larger FVC is automatically substituted. Realistically however, this approach is just as likely to introduce errors into the calculation of TLC and RV it’s just that I think the errors are easier to detect.
References:
Brusasco V, Crapo R, Viegi G. ATS/ERS task force: Standardisation of lung function testing. Standardisation of the measurement of lung volumes. Eur Respir J 2005; 26: 511-522.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License