One of our testing systems has been leaking during the breath-holding period of DLCO tests. This has been an on-again, off-again problem caused by a leaking balloon valve. The odd thing about this is that the results from tests that show a patient leak are often higher than the results where they don’t.
This is not the pattern I would have expected. My initial thought would be that in the DLCO tests with a leak, the patient is spending more time at a lung volume below TLC which in turn means a lower surface area. A lower surface area should lead to a lower DLCO but this doesn’t appear to be happening.
Here are two DLCO tests from a young female patient with average height and weight. She had a normal TLC and mild airway obstruction.
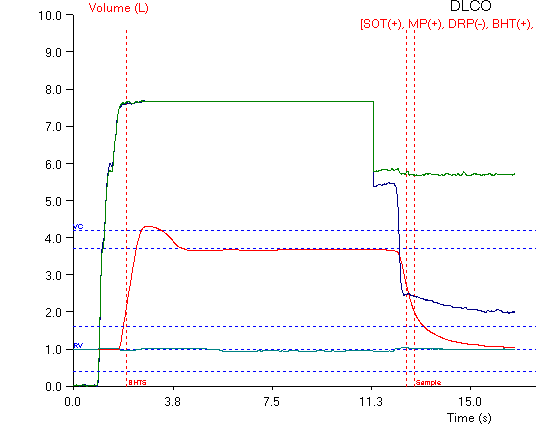
DLCO test with a leak during the breath-holding period
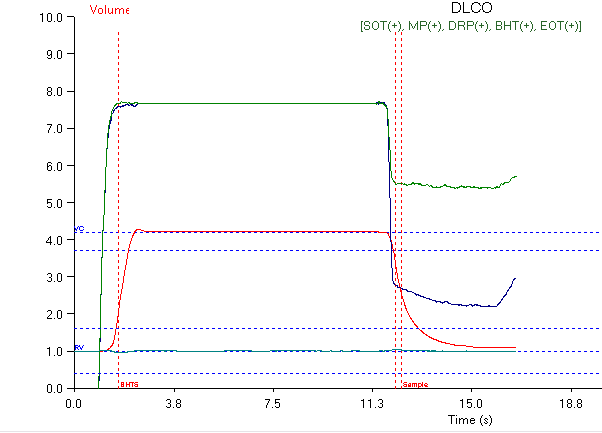
DLCO test from the same patient without a leak
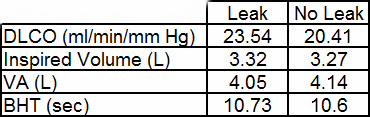
The DLCO results from the test with the leak are 15% higher than they were from the test without the leak. There is no significant difference whatsoever in Inspired Volume, VA and breath-holding time between the two tests.
I first noticed this problem a number of years ago but I was never able to reproduce the results despite numerous trials on myself so I was never sure what to make of it. This problem only showed up rarely so I just left it as one of those mysteries you run across once in a while.
Recently however, a much larger number of patients are showing this oddball pattern of higher DLCO results when they leak than when they don’t. The only significant difference is that when I noticed this previously our test systems were all based on a volume-displacement spirometer and now we have several pneumotach-based systems capable of DLCO testing.
All of the recent (and more plentiful) examples are coming from our pneumotach-based test systems. One reason why we’re noticing this problem more frequently on these systems than we were on our volume spirometer systems may have to do with the fact that on the volume systems there were two opening in the breathing manifold that a patient could exhale through. Both had balloon valves, but if the balloon valve to the spirometer was not leaking while the other one was, then the leak would not be detected. The only time a patient leak would be detected was when the balloon valve to the spirometer was leaking. On the pneumotach-based test systems there is only one valve and any leaks around the balloon valve can only go through the pneumotach and are therefore always detectable.
Assuming that the cause of the difference in the test results is physiological there is only one thing that can elevate DLCO results and that is an increase in pulmonary capillary blood volume. Since the patients didn’t go anywhere or do anything in particular between tests an increase is unlikely to come from an increased cardiac output from exercise. A Mueller maneuver (inhaling against closed mouthpiece) causes a negative airway pressure which can pull blood into the lung and increase the pulmonary capillary lung volume. A Mueller maneuver is a difficult maneuver to perform however, and most patients are far more likely to perform some variation on a Valsalva maneuver which raises airway pressure and decreases both cardiac output and the pulmonary capillary blood volume.
One possibility however, is that the patients are performing a Valsalva maneuver at the start of the breath-holding period but that when they leak their airway pressure decreases enough to allow their cardiac output to rebound and their pulmonary capillary blood volume to increase. Even though the lung volume decreases from TLC due to the leak, this probably doesn’t decrease surface area enough to make a difference, or if it does, the increase in pulmonary capillary blood volume may be greater than any decrease in surface area.
The fact that there is a possible physiological mechanism to explain these results does not rule out other errors in the measurement process but at the moment I have difficulty seeing what they could be. I was never able to reproduce this problem on myself however, so there may well be other factors at play here.
I think that the most important take-away from this problem is that errors in the testing process can cause increases in DLCO results as well as decreases. This means that you can never assume that a higher DLCO test result is better or more correct than other results and that DLCO test results should always be inspected carefully before they are reported.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.