A couple days ago I pulled my copy of the Intermountain Thoracic Society manual on pulmonary function testing off the bookshelf and thumbed through it a bit. It was first published in 1975 and was the first major attempt towards standardizing the performance and interpretation of PFTs.
My first thought was that we’ve come a long way since then. Most importantly our understanding of what spirometry can (and cannot) tell us has improved dramatically.
Equipment too, has advanced since 1975, most particularly due to the first equipment standards that were published in that decade. As a reminder, spirometer accuracy was not a given and there are number of studies dating from that time period that detailed just how woefully inaccurate many of them were.
In 1975 computerized spirometers were exceptionally rare and I was reminded of this because 141 pages (two-thirds!) of the ITS manual is filled with look-up tables for predicted values and ATPS – BTPS – STPD conversion factors.
Most spirometry systems were entirely manual and the majority of us measured FVC and FEV1 manually from pen tracings on kymograph paper. The results were then hand-calculated and then hand-written onto report forms. Since our equipment is so much more accurate and our computers acquire and calculate test results automatically, everything is so much better now, isn’t it?
Overall, I’d have to say yes. Testing is much quicker and more accurate than it used to be in 1975, and no, I’m not particularly nostalgic about those days.
{Arrrhh, gather round lads and lasses and let me tell you of the days when coal-fired steam-powered spirometers rumbled and hissed in basement labs everywhere; when you had to solve regression equations with your slide rule on the fly or risk the horror of ripped kymograph paper, exploding alveolar sample bags and spirometer bells gone ballistic without warning. The toll this daily physical and mental trauma took amongst the lowly pulmonary techs was terrifying and only the bravest continued the daily battle against gnarly patients, sneering doctors, black-hearted administrators and monopolistic manufacturers…
…Oops! Wrong time-line; those are memories from the universe one north and two left of ours. Too much steampunk sci-fi late at night and too little sleep left me momentarily confused…}
I ran across an error today that reminded me that although computerized test systems are essential to our ability to run efficient and accurate labs, at the same time the limitations of software that comes along with them hinders our ability to detect and correct errors.
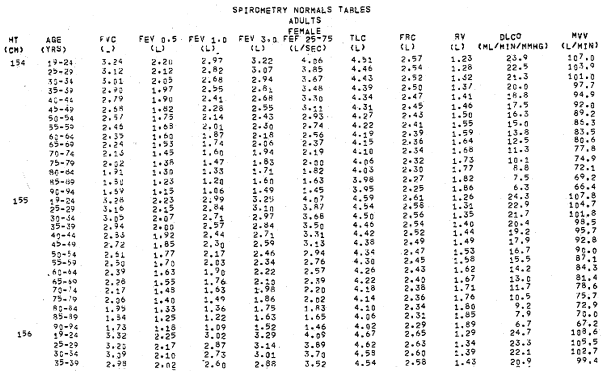
A patient’s spirometry results came across my desk and every effort had excessive back-extrapolation (ranging from 0.33 L to 0.56 L). The tech performing the tests had indicated this in the notes but when I took a close look at the volume-time curves I was somewhat baffled since the beginning of each spirometry effort was sharp and clearly evident.
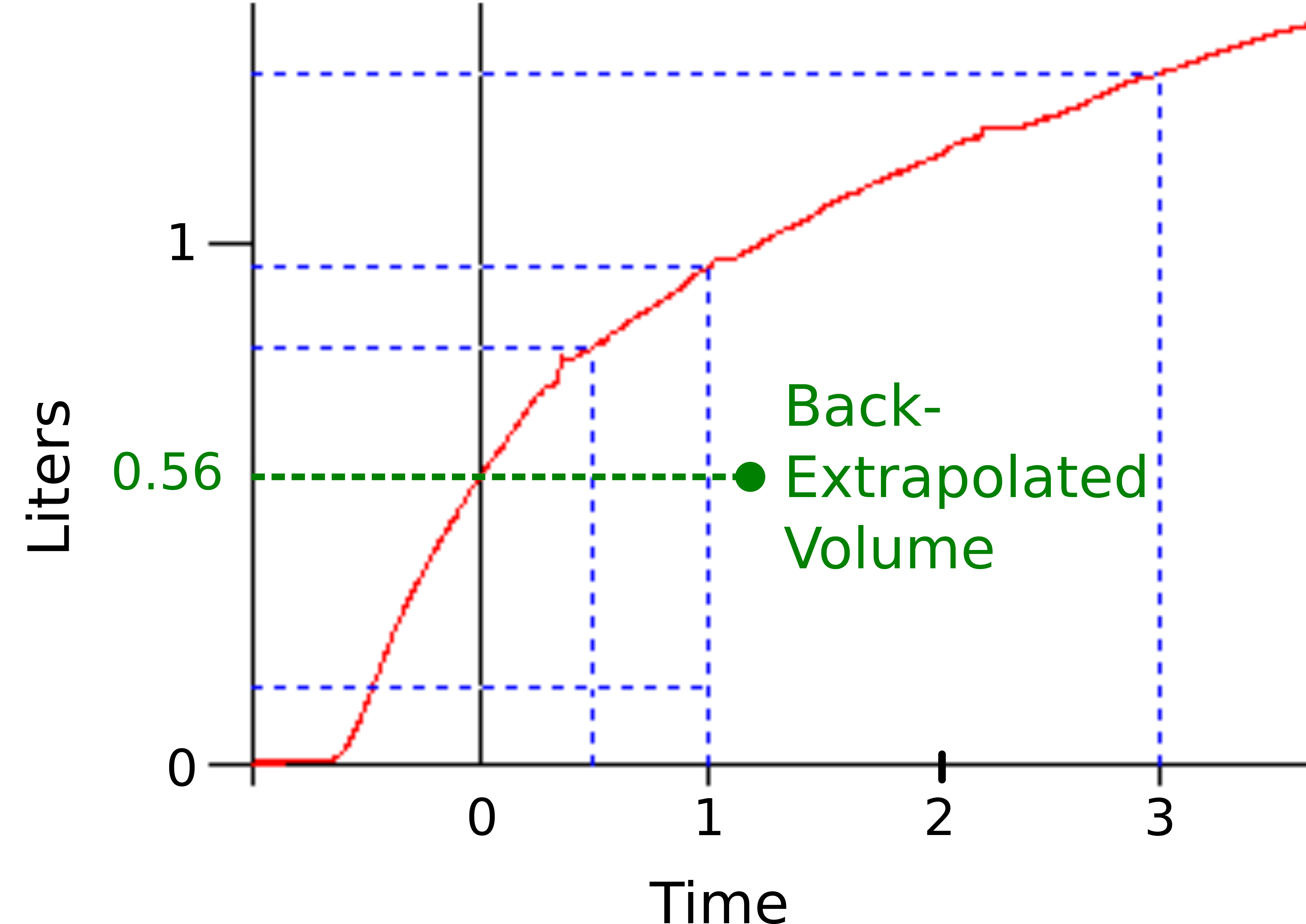
It was only when I looked at the flow-volume loop that I realized what was happening.
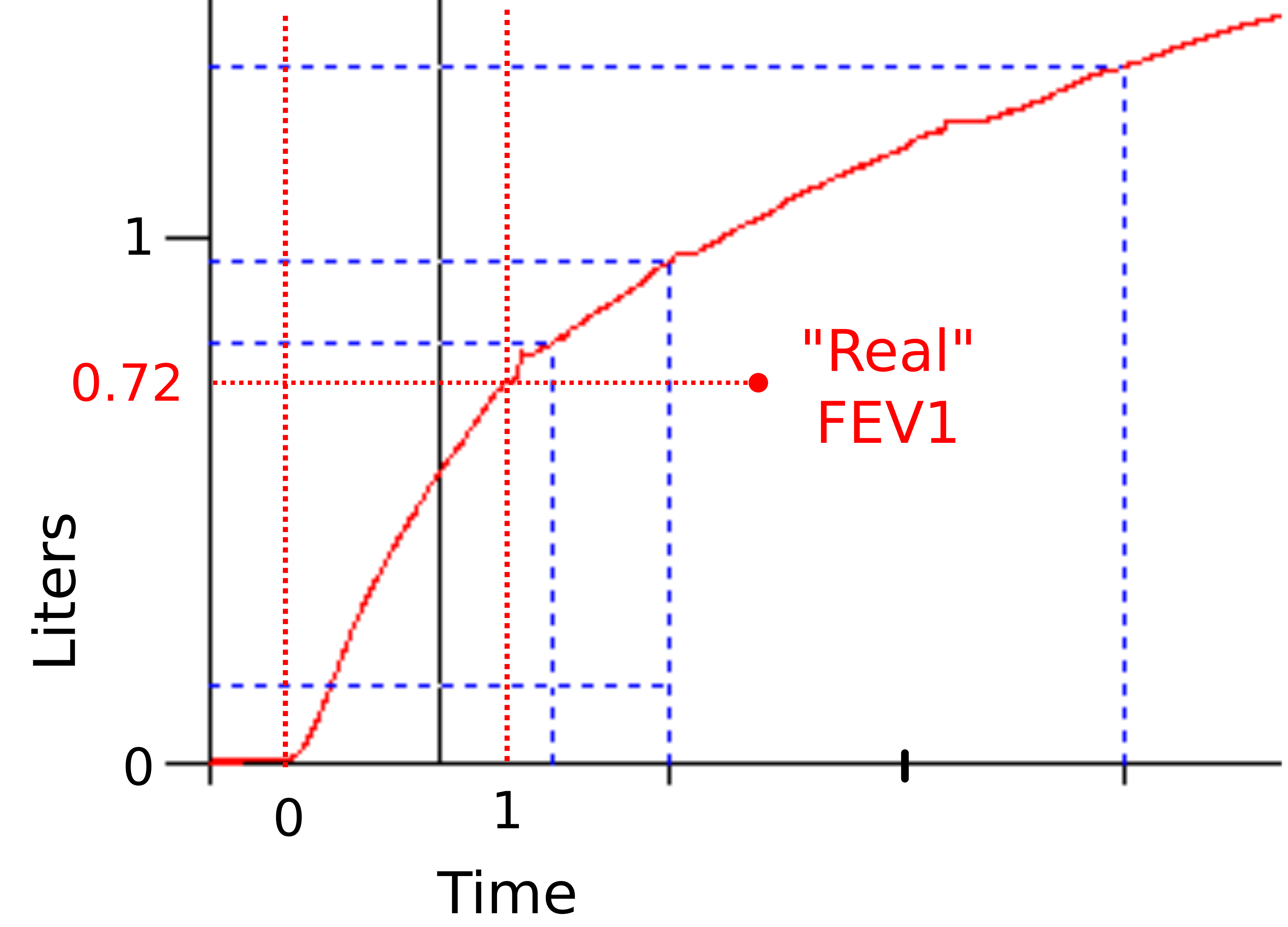
The back-extrapolation algorithm has it’s basis in the volume-time curve. Back in the day, you used a ruler to find the highest slope of the volume-time curve and used it to extrapolate backwards to the “real” beginning of the expiratory effort.
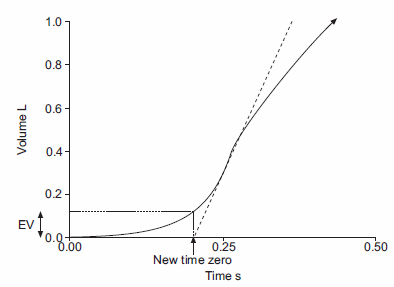
From ATS/ERS Standardisation of spirometry, Figure 2, Page 324
The highest slope however is, by definition, the peak flow. Computer software uses this fact to look for the peak flow and uses this to perform back-extrapolation. In this case, the patient was coughing during each expiratory effort, and in each effort, this cough caused expiratory flow to spike above the “real” peak flow for a very short interval.
This “spike” was used by the computer algorithm to determine back extrapolation and because it was using the wrong “peak” flow, it was mis-calculating both the FEV1 and the amount of back-extrapolation.
If the “real” start of exhalation was used instead, the FEV1 changes from 0.96 L (37% of predicted) to 0.72 L (28% of predicted), and although that’s a relatively small difference it changes the interpreted severity of the patient’s airway obstruction from “severe” to “very severe”.
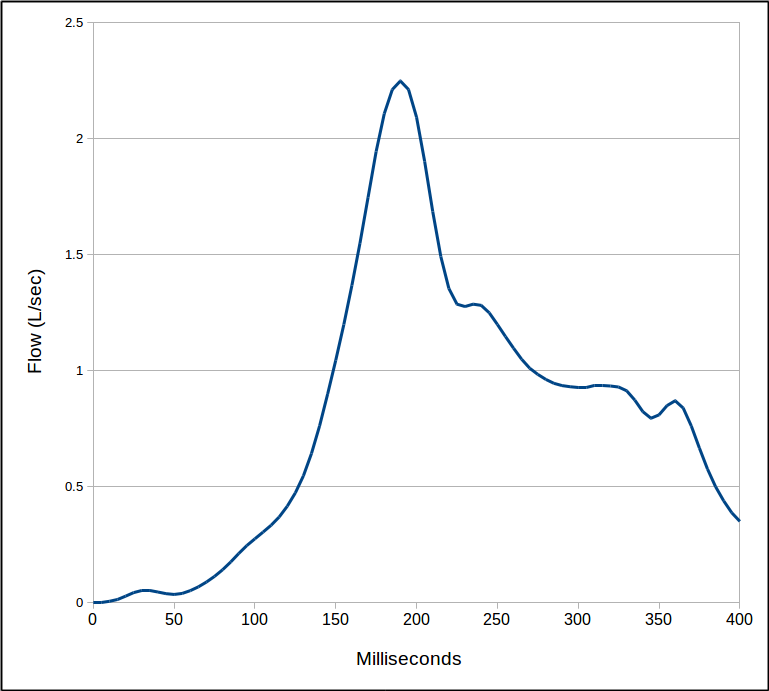
There are, of course, at least a couple things wrong with this. First, you’d think after all these years that software could account for coughs and ignore them. The cough in this instance lasted only 35-40 milliseconds.
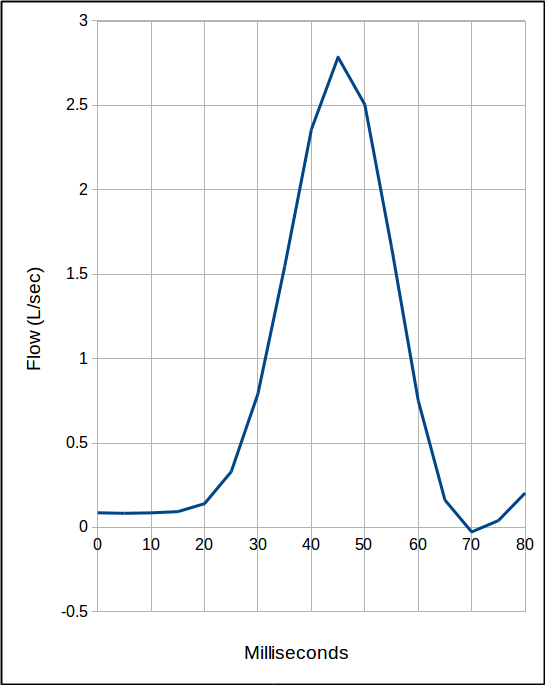
The “real” peak flow, on the other hand, lasts 100’s of milliseconds.
Second, I have no way to correct this error, other than mentioning it in the notes. Our lab software lets me make at least some corrections to our DLCO tests and lung volumes, but for spirometry the best I can do is to select the computer-measured FVC and FEV1 from different efforts.
Third, this error is relatively obscure and hard to detect. It would have been much more evident if the back-extrapolation process had been visually graphed but this type of graph is not available from my lab’s software and it only reports back-extrapolation numerically.
So, yes, computerized test systems have made spirometry faster and more accurate than it was back in 1975 but only when the software algorithms are correct, and this is not always the case. My concern is that errors like this (and there are probably more that occur with some kind of regularity) are difficult to detect and in many cases, impossible to fix.
I don’t see any easy solution to this problem. Equipment manufacturers have no particular incentive to find and fix these problems (that’s not to say that there aren’t some that are at least trying but in the current PFT and spirometry marketplace there’s no real payback for these kinds of efforts). I can say with some assurance that the spirometry algorithms in my lab’s software have remained unchanged for at least the last 12 years, and that they are probably directly based on software algorithms from the 1980’s and 1990’s.
Manufacturers do respond to regulation and standards. The ATS/ERS spirometry standards have done much to improve spirometry quality but there are notable gaps in their recommendations that are left to individual manufacturers to interpret and solve. In addition the spirometry guidelines are now 13 years old and there is no particular sign that new ones are being developed (and from discussions I’ve had with other PFT veterans there’s no indication that even if they were that they’re soliciting input from any of us in the field).
My real point however, is that by using computerized testing systems (not that that there’s been any alternative for at least a couple decades) we’ve traded some of our autonomy for convenience and productivity. Most of the time this is probably an acceptable trade but every so often we’re going to pay for this by (knowingly or not) reporting inaccurate results.
Despite all this it’s your responsibility to move brightly into the future and interact in a positively rewarding manner with your grateful patients, knowledgeable physicians, generous administrators and enlightened manufacturers…
[…Oops! Wrong universe again! That’s the one that’s three south and one rightwards of ours…]
References:
Brusasco V, Crapo R, Viegi G. ATS/ERS task force: Standardisation of lung function testing. Standardisation of spirometry. Eur Respir J 2005; 26: 319-338.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International Lic
Your storytelling sequence reminded me of something that actually did happen: the spiro bell going ballistic, or at least as far as the chain on the Stead-Wells spriometer would let it go. It was right after I’d gotten a Godart FRC ‘computer’, and the He had to be bled in by hand, and attention paid to when 1 L. had been reached. The phone rang, attention shifted, and a bit of excitement ensued in the lab.
Mike –
I had my share of incidents as well. I started work the Collins Modular Lung Analyzer that had the two weather balloons in the plexiglass box underneath. More than once I got distracted while filling the inspiratory bag with the DLCO gas and ended up breaking the box (with a loud bang) when the balloon over-filled. Got pretty good at re-gluing the box. One the reasons that I learned a lot about PFT equipment is that I broke a lot of it along the way.
Regards, Richard
A few posts back you got a comment from Ralph Stumbo, in the Puget Sound area. Next time you correspond with him tell him ‘hello’ from me. Ralph worked with me decades ago, and he was one of the more apt people I’ve know in picking up the craft. A all around good guy.
Mike
This is a very interesting observation. The results of this testing are not informative. The work of the software is designed for certain criteria. these are the quality criteria described in the previous article. The presented test has a low level of quality, and therefore in its interpretation there may be inaccuracies. It is possible to solve the problem by properly performing the test, for example after treatment ….
Andrey –
The patient coughed and caused excessive back extrapolation in all four attempts. Yes, I’d agree that test quality wasn’t perfect, but coughing happens all the time during spirometry so why haven’t the software manufacturers been able to figure out a way around this? The fault isn’t with the patient, it’s with the software.
Regards, Richard
Wouldn’t it be lovely if we did live in the universe that’s three south and one rightwards of ours 🙂 Thank you again for all your tireless effort keeping us informed & entertained! You have managed again to nearly take the words right out of my mouth, equipment manufacturers seem to have no particular incentive to fix these problems even after you point them out (i would have thought inaccuracy would have been a strong motivator but it doesn’t appear to be). Your blog is a true gem for all respiratory technicians around the world.