The Global Lung Function Initiative (GLFI) was established by the European Respiratory Society in 2008 with the goal of establishing a truly worldwide set of reference equations for spirometry. Its results were released in the December 2012 issue of the European Respiratory Journal. Although the reference equations presently apply only to Caucasians, African-Americans and northern and southern Asians, it will likely be updated with Hispanic, African and Polynesian data within the next couple of years.
This has been a massive undertaking involving spirometry data from 72 different testing centers in 33 countries. The data has been subjected to rigorous quality control and an extensive, sophisticated statistical analysis and will likely become the standard reference equation set for spirometry testing in Pulmonary Function labs around the world.
The reference equations are quite complex, if for no other reason than that they cover an age range that encompasses young children to the elderly (age 3-95). I have a limited background in statistics and find it difficult to understand how the various factors in the equations were developed and how they work together. The best I can do is to compare the GLFI predicted values to the reference equation my lab is presently using, NHANESIII. Starting with adult male and female Caucasians of average height, there are several apparent differences.
It is evident that the GLFI reference equations describe a more complex relationship between age and spirometry values than does NHANESIII. The NHANESIII reference equations are simplistic in that they are regularly curvilinear for FVC and FEV1 and show an accelerating decline in these values with increasing age. Even more so for the FEV1/FVC ratio that is entirely linear and shows a steady decline with age. In comparison, the GLFI reference equations for FVC shows that the maximum FVC volume for both males and females is attained in their mid-20’s whereas NHANESIII shows it peaking around age 20. Similar to NHANESIII the GLFI shows an accelerating decrease in FVC up to middle age, but then shows a period of linear decrease up to about age 75 and finally a decelerating rate of change thereafter. For FEV1, the GLFI reference equations show a similar, although somewhat subtler pattern to that of FVC and like NHANESIII, FEV1 peaks around age 20. For the FEV1/FVC ratio, both NHANESIII and GLFI show approximately the same trajectory up until middle-age, when the GLFI starts to decrease less rapidly than NHANESIII.
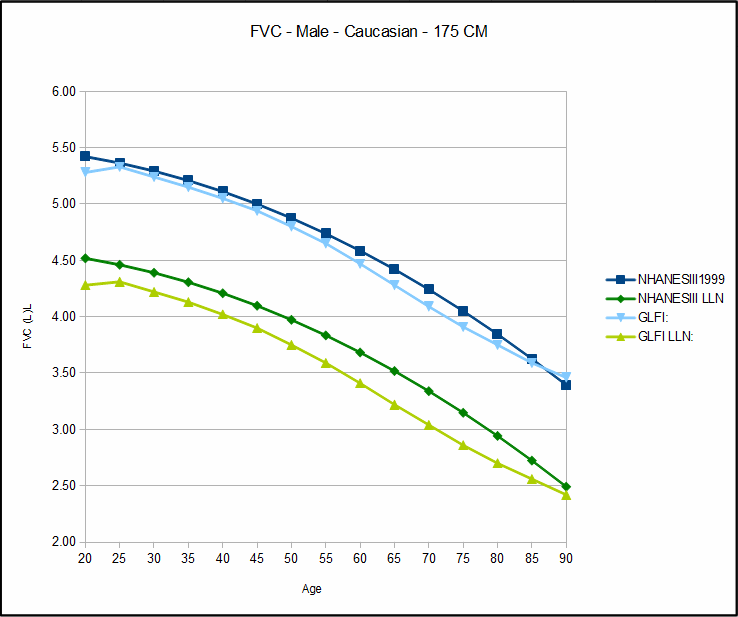
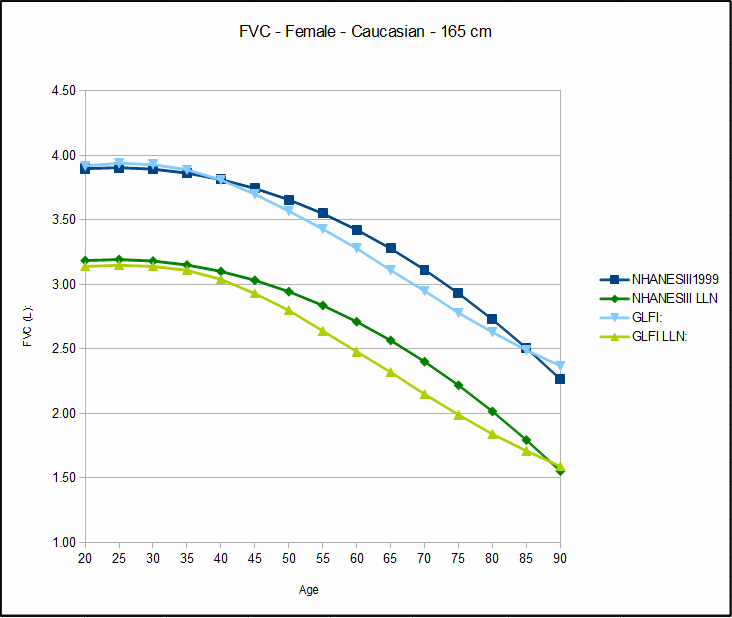
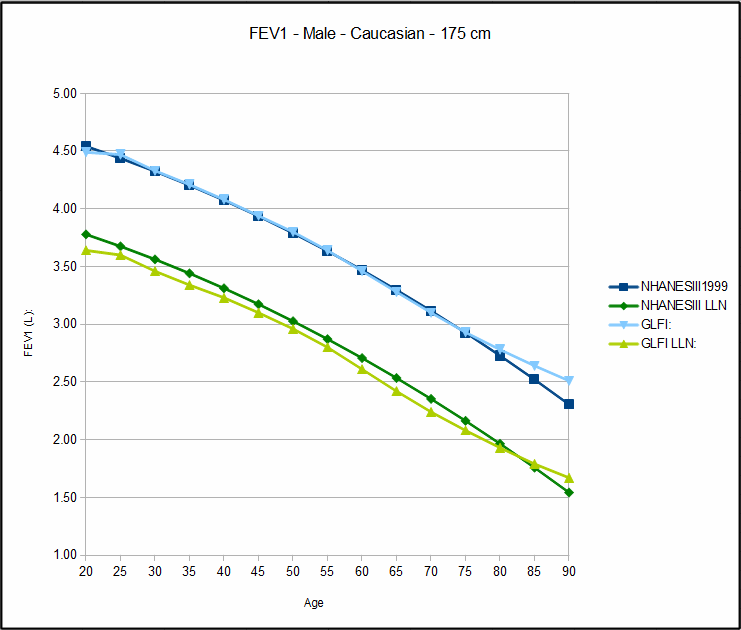
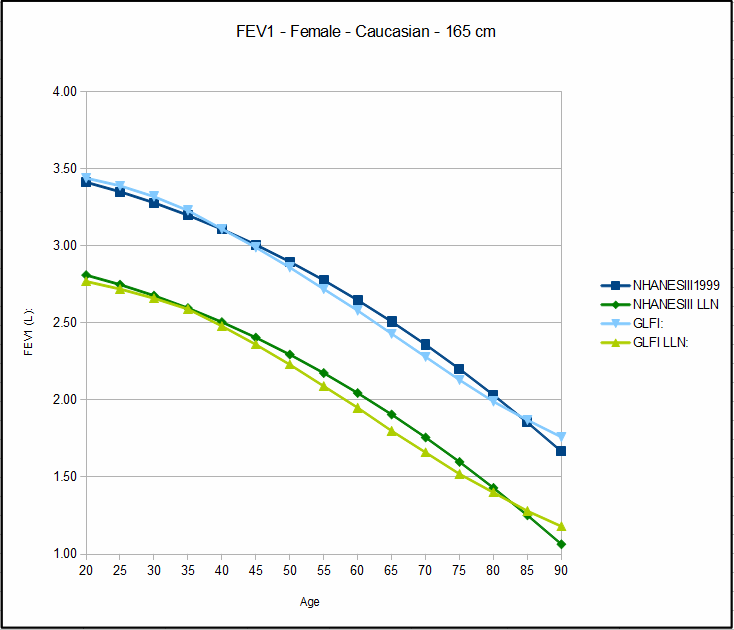
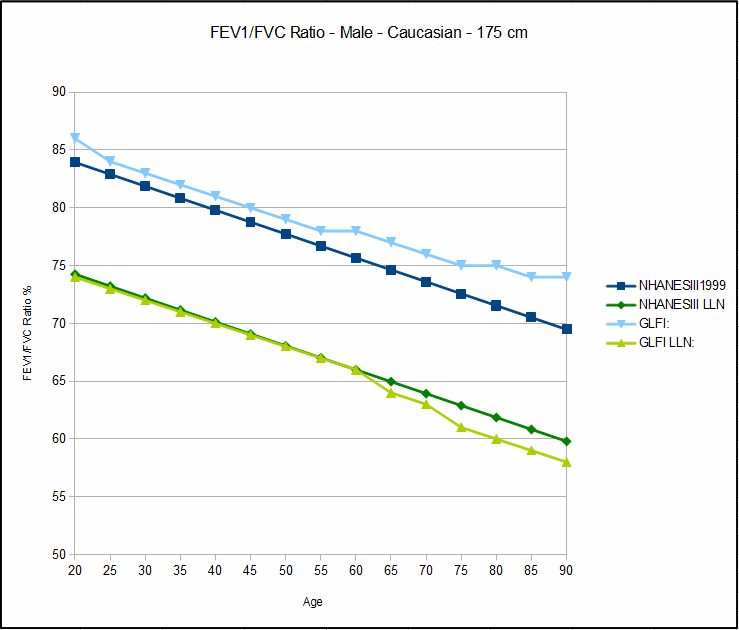
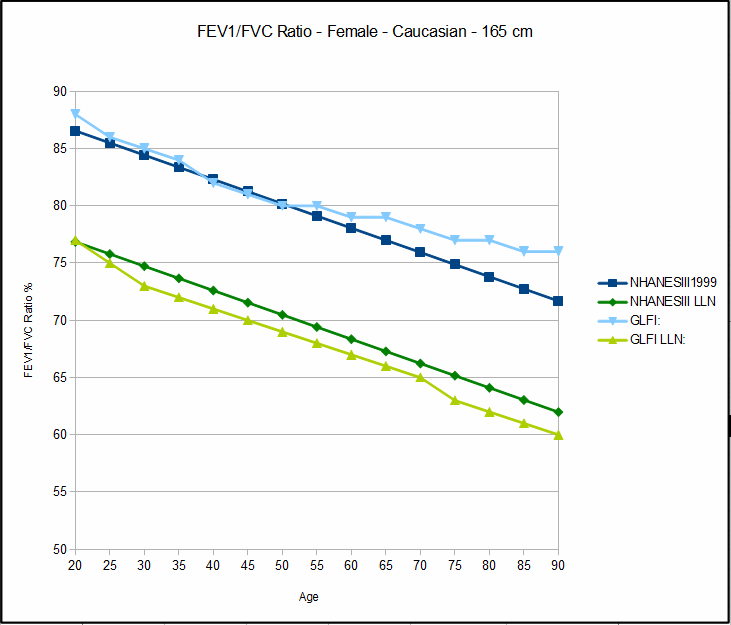
The practical consequences of switching from NHANESIII to GLFI would be that more patients would be considered normal. This is partly because the predicted FVC and FEV1 values tend to be lower for GLFI than they do for NHANESIII. It is also because the lower limit of normal (LLN) for GLFI is lower both in an absolute sense and because there is a larger spread between the predicted values and the LLN. This larger spread of LLN is particularly true of the FEV1/FVC ratio because even though the predicted ratio is higher for the elderly than it is for NHANESIII, the LLN is strikingly lower.
One implication of this would certainly be that in particular fewer elderly patient would be diagnosed with obstructive lung disease. It also implies that airway obstruction is less prevalent in the general population than currently thought. Having said that I continue to have reservations about the use of LLN primarily because I think it sets the bar too low but since it appears that LLN is well on its way towards becoming a worldwide standard, I will probably just have to live with this.
I don’t think there is much doubt that the GLFI reference equations will become the worldwide standard for spirometry testing. Creating the GLFI equations was a monumental undertaking requiring a data set of over 97,000 spirometry records from around the world that were subjected to rigorous quality control and statistical analysis. In contrast, the prior gold standard for spirometry testing, the NHANESIII study, contained only 7429 spirometry records, primarily from an American population.
The GLFI data set will no doubt be mined by researchers and statisticians for some time to come. I think one of the most important contributions the GLFI makes is that what it is telling us about lung function and age is much more likely to be true than any prior study has been able to.
Although the GLFI sets a new standard for spirometry reference equations, it remains an evolving process. At the very least it still needs to be fleshed out with data from more ethnicities before it can be considered to be in any way complete. Along those lines, I would like to see more guidelines about determining ethnicity given that ethnicity is too often a matter of opinion rather than physiological fact. I would also like to see more longitudinal studies that attempt to verify how well the LLN actually matches reality.
You can download Excel spreadsheets and Windows software for exploring the GLFI equations from the GLFI website.
References:
Hankinson JL, Odencrantz JR, Fedan KB. Spirometric Reference Values from a sample of the general U.S. Population. Am J Respir Crit Care Med 1999; 159: 179-187.
Quanjer PH, Stanojevic S, Cole TJ, Baur X, Hall GL, Enright PL. Hankinson JL, Ip MS, Zheng J, Stocks J. Multi-ethnic reference values for spirometry for the 3-95 year age range: the global lung function 2012 equations. Eur Respir J 2012; 40: 1324–1343.