We’ve been aware of this particular issue for several years. My PFT lab has had some turnover lately and the newer staff aren’t familiar with this problem so it has re-appeared in some of the reports I have been reviewing.
Our lab has a mix of flow-based and volume-based test systems. This problem is peculiar to only the volume-based systems that have a vertically mounted volume-displacement spirometer and is due in part to mechanical issues but also to some underlying assumptions made by the test software.
During the set-up process for a DLCO test, the spirometer bell and the systems tubing and patient manifold are first flushed and then the spirometer bell filled with the DLCO test gas mixture. The balloon valves in the patient testing manifold are then closed to keep the spirometer bell in position and do not open again until the start of the DLCO test.
It is usually obvious if any of the balloon valves in the manifold are leaking. Either the testing system cannot complete the set-up process or the spirometer bell can be seen to be dropping when it should be remaining stationary. This requires that the balloon valve have a fairly significant leak, however, and a small leak may not be so evident.
Usually we have the patient perform the DLCO test as soon as the set-up is done. When this is the case a small leak has little effect on the DLCO test. Occasionally however, and for any number of good reasons (the patient has to go the bathroom or wants a drink of water, etc.) there may be a prolonged period between set-up and testing. When this period of time is long enough there may be a significant leak from the spirometer bell even when the balloon valves have passed all of our regular leak tests.
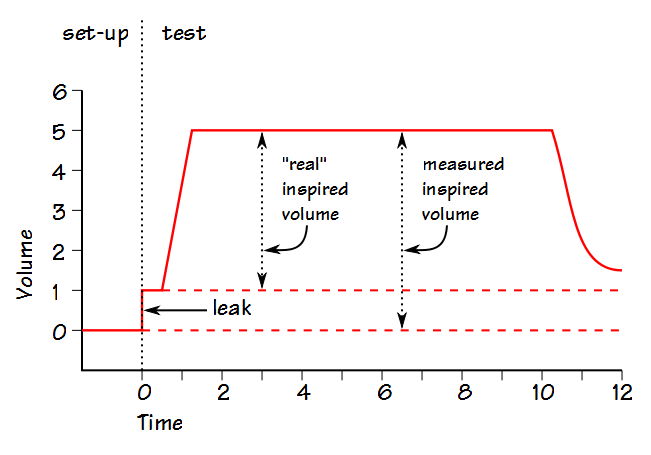
The problem occurs because the test software assumes that the position of the spirometer bell at the beginning of the DLCO test is the same as it was at the end of the set-up process. For this reason, when there is a leak and the spirometer bell position drops the inspired volume will be overestimated because the software does not take into account the new position of the spirometer bell. Since Alveolar Volume (VA) is a function of inspired volume:

VA will be overestimated when the inspired volume is overestimated. Since the calculated DLCO scales with VA:

this means that DLCO will be overestimated when the inspired volume is overestimated (and vice versa).
The lab equipment is regularly tested for leaks, but valves can (and all too frequently do) fail. Tubing can also develop leaks and any of these leaks can run the gamut from large and obvious to small and subtle. The work-around for this problem has been first to make the staff aware it can happen and what effect it has on the DLCO test (as well as lung volumes and spirometry, of course). Second, either to always perform the DLCO test shortly after the set-up has finished or if too much time has passed before the patient is ready to perform the test, abort it and start over.
The real solution would be to have the DLCO testing software re-check the position of the spirometer bell at the beginning of the test and either re-establish the zero volume baseline or stop the test if the bell has dropped too far. This error was passed on to the manufacturer of our test equipment when we first noticed it but so far a fix has not appeared in our software updates.
This problem is unique, as far as we can tell, to our volume-based testing systems. A larger point though, is that anything that can cause the inspired volume to be mis-measured and either over- or under-estimated will have a corresponding effect on the calculated DLCO. We do not see baseline shifts in our flow-based test systems but that doesn’t mean that inspired volume hasn’t been underestimated during the test itself due either to a patient or system leak (on these systems I have a lot of trouble seeing how inspired volume could be over-estimated other than with a mis-calibrated pneumotach). When I review DLCO test results I often see inspired volumes that are less than the FVC, sometimes substantially so. That may be just because that is the way the patient performed the test but unlike the pre-test leak with our volume-based test systems there is nothing particularly evident about a leak during inhalation.
Leaks are the bane of a Pulmonary Function Lab’s existence. They are a chronic problem and any lab that doesn’t think it has a problem with leaks probably isn’t looking hard enough. Depending on when and where they occur leaks can cause the results from any test to be over- or under-estimated. The only answer is to be familiar with your equipment’s failure modes and how they show up in test results. Having said all of this, I also have to say that equipment manufacturers often don’t make it particularly easy to determine if their test equipment is leaking or to find the source of the leak. From the equipment manufacturers point of view, as long as a leak isn’t from a manufacturing flaw it’s not their problem. I would argue that more care should go into valve design and the ability to more rigorously test for leaks, but these don’t seem to be factors that sell test systems and that’s at least partly our own fault.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.