While reviewing reports today I ran across a couple of lung volume tests from different patients where the SVC was over a liter less than the FVC. Suboptimal SVC measurement can affect both the TLC and the RV and in one case the TLC was slightly below normal (78% of predicted) and in the other the TLC was within normal limits but the RV was over 150% of predicted. Both patients had had lung volume measurements previously and the current TLC was significantly different than it had been before.
I seem to run across this problem at least once a week so I am reasonably used to making manual corrections. I’ve discussed this previously but basically I use the position of the tidal loop within the maximal flow-volume loop obtained during spirometry to determine IC and ERV and then re-calculate TLC and RV accordingly.

Anyway, for this reason I had tidal loops, and IC and ERV on my mind while I was reviewing other reports. Shortly after this I came across a report that had “fair FVC test quality and reproducibility” in the tech notes so I pulled up the raw spirometry test data and took a closer look.
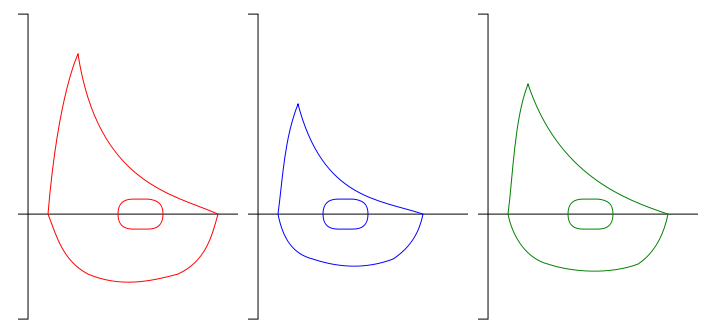
What I found was that the patient had performed five spirometry efforts and that the FVC and FEV1 was different on each test. All five spirometry efforts met the ATS/ERS criteria for back-extrapolation, expiratory time and end-of-test flow rates. I clicked back and forth between the different spirometry efforts to make sure the right FVC and FEV1 had been selected and when I did I noticed that the position of the tidal loop was shifting left and right and that the closer it was to TLC, the lower the FVC and FEV1 were and vice versa.