The most common problem we have with helium dilution FRC tests are leaks. Although the system tubing and spirometer bell leak occasionally, we do have valve failures relatively frequently. Valve failures are usually obvious but they sometimes only fail partially so leak checks are regularly performed on these test systems. We can’t perform leak checks on patients except while they are being tested however, and patient leaks are far more common than system leaks.
A technician asked me to look at a patient’s helium dilution FRC test because it had an odd helium tracing. The technician was sure the patient had been leaking but the FRC from this test was was actually the lowest of three tests and they weren’t sure why that was the case.
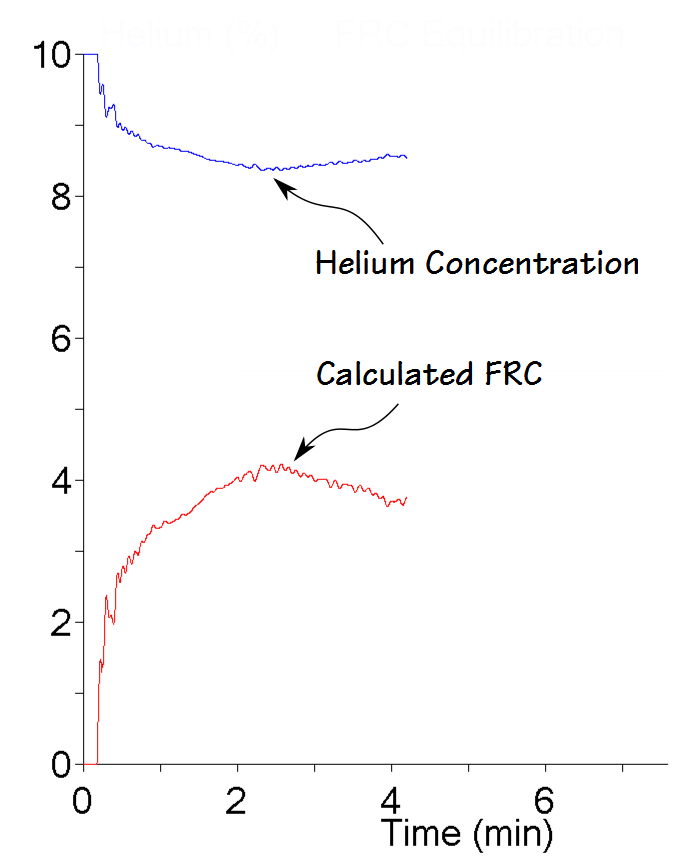
Once I saw it I was immediately able to tell the technician that it wasn’t a leak and that it was probably okay to report the results. I was able to say this because when there is a leak during a helium FRC test the helium constantly decreases and never plateaus. The rate of decrease may change but the most pertinent point is that the helium concentration never plateaus and even more importantly, it never increases.
I’ve seen this particular type of helium tracing before but to be sure I could properly explain what caused it I downloaded a table of system readings from the test software and they verified that what I thought happened was probably correct.
A bit of background first. A helium dilution FRC is measured using a closed-circuit technique.
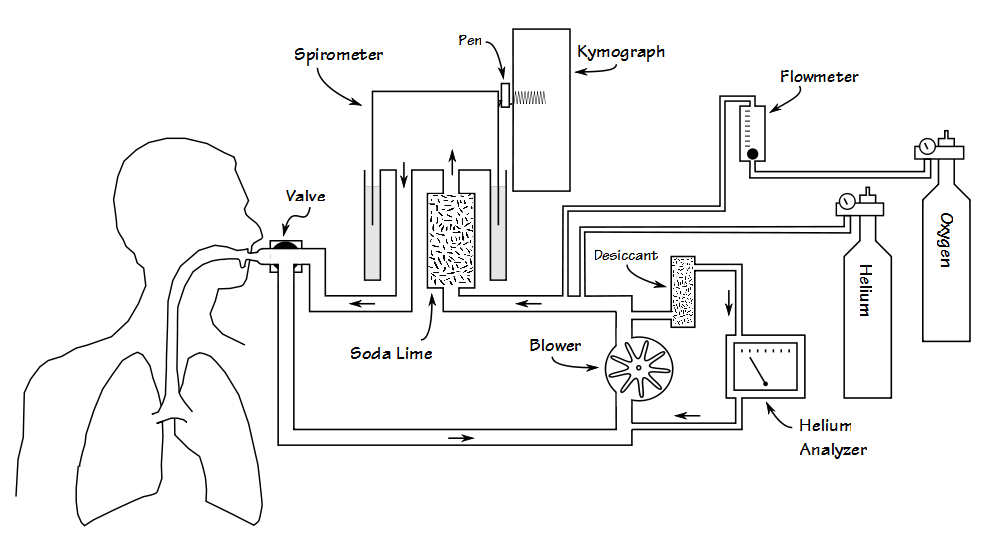
Well over a hundred years ago it was realized that carbon dioxide was a potent respiratory stimulant and for this reason when a patient breathes in a closed circuit exhaled carbon dioxide has to be removed. Several different (and hazardous) chemicals were tried for this purpose but it was discovered that soda-lime was very effective at doing this and soda-lime has been used for this purpose ever since. (An interesting historical side note is that the first measurements of the rate of exhaled carbon dioxide production was performed by measuring the weight of soda-lime before and after it had absorbed carbon dioxide.)
One of the first clinical uses of a closed-circuit spirometer system was to perform basal metabolism testing by measuring oxygen consumption. This was done by filling a closed-circuit with oxygen and having a patient breathe for an extended period of time. Since all of the patient’s carbon dioxide was being absorbed, the decrease in circuit volume could only occur because of oxygen consumption. This kind of testing was performed first in Germany in the 1890’s and was brought to the United States before 1910. By the 1940’s the volume decrease due to oxygen consumption was a well documented and understood consequence of closed-circuit testing.
The first helium dilution FRC test was performed in the mid-1940’s. It used the same principle as a hydrogen dilution lung volumes test first performed in the 1930’s. Both helium and hydrogen are relatively insoluble gases. When a gas is insoluble only small amounts of it are absorbed by the blood or lung tissue and this makes it useful as a tracer gas. Helium is more insoluble than hydrogen and it is relatively easy to measure accurately, and it is for these reasons that it became a standard way to measure lung capacity.
Measuring lung volume with helium requires that the volume of the closed-circuit system remains constant. Since carbon dioxide is being absorbed and oxygen is being consumed this means that oxygen needs to be added throughout the test. The question then becomes how do you know how much oxygen to add?
When I started performing pulmonary function testing with manual systems the practice was to use the kymograph pen to draw a horizontal line where the patient’s end-exhalation (FRC) would be once the system had been set up for the test. Once I switched a patient into the circuit at end-exhalation I would set the oxygen flow meter for around 350 ml/min and then watch where their tidal breathing was relative to the line I’d drawn. If they rose or fell from the baseline I’d decrease or increase the oxygen flow rate. The idea was that at the end of the test, the patient was still on the baseline.
When computerized systems came along basically the same technique was used. The patient’s end-exhalation level is measured at the start of the test and oxygen is added (usually in pulses, not continuously) whenever the patient dropped below the baseline. When I added added oxygen manually there were times when I did better at it and times when I did worse. What I quickly learned was that there were a number of subtle things like the patient shifting their position in the chair or changing their breathing pattern (patients often hyperventilate at the start of a test and slow down later in the test) that could change their FRC baseline. Sometimes tests went longer than they “should have” because I added too much oxygen, “overshot” their FRC baseline and then had to wait for the patient’s oxygen consumption to return them to it.
The same problems occur when patients are tested with a computerized system as when they were tested on a manual system. When I reviewed the information for the FRC test with the odd helium tracing what I saw was that a modest amount of oxygen was being added during the first minute of testing but during the next minute or so the amount of oxygen being added to the circuit went up dramatically. During the final minute and a half or so the amount of oxygen being added decreased to a more or less normal level and stayed there until the end of the test.
So what likely happened was that the system added too much oxygen during the second minute of the test and “overshot” the patient’s FRC baseline. This diluted the helium in the breathing circuit and caused the dip in the helium concentration. It then took almost two minutes for the extra oxygen to be consumed and the helium concentration to return to its “real” level. Unfortunately, the test software doesn’t store any of the volume information from the test, so I couldn’t actually see if this what happened but I think this scenario fits the facts best.
But even if I’m wrong it still wasn’t a leak.

PFT Blog by Richard Johnston is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.