I was reading an article recently that made an off-hand reference to the 100% oxygen shunt fraction test. Results from the test were included in the data analysis but the equations the researchers used were not presented nor were they referenced, nor was the procedure described. This is probably because the shunt fraction test and its equations are very much old-school pulmonary physiology but even if the subject is probably covered at one time or another in physiology classes I suspect that some of the issues involved in the calculation are not as well understood as they should be.

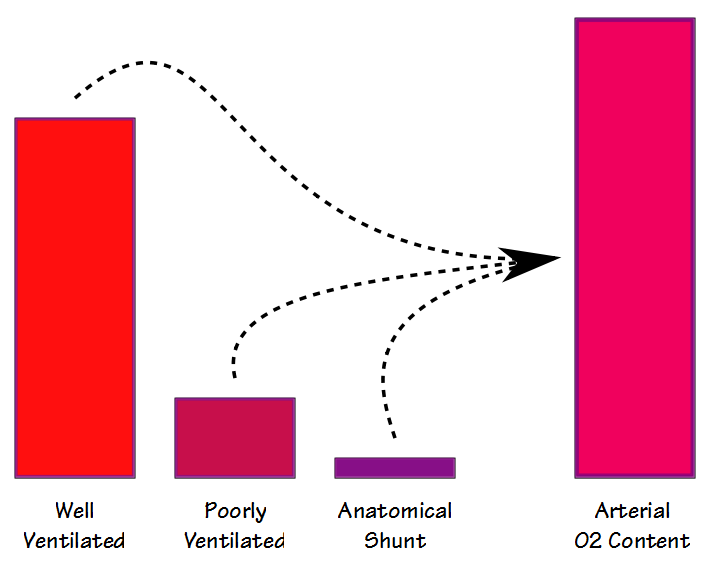
There are some similarities between the deadspace-tidal volume ratio (Vd/Vt) and the shunt fraction but even though they are both are involved in gas exchange (and to some extent they also correlate with each other) they are measuring different things. When blood flows through the lung some blood passes through well ventilated alveoli and becomes fully saturated; some blood passes through poorly ventilated alveoli and is only partially saturated; and some bypasses the alveoli entirely. The resulting arterial oxygen content is the summed average of all of these compartments.
There are two different ways that shunt fraction can be measured and calculated; physiological and anatomical. The physiological shunt equation can be performed at any FiO2 (but usually around the FiO2 of room air) and requires that arterial and mixed venous blood samples be taken more or less simultaneously and then analyzed for PO2 and SaO2. The basic formula is:
![]()