Two PFT reports came across my desk recently and comparing them got me to thinking about Peak Expiratory Flow (PEF). The FEV1 from both tests were mildly reduced with an FEV1/FVC ratio that was moderately reduced and an FVC that was within normal limits.

| Observed: | %Predicted: | |
| FVC (L): | 3.72 | 96% |
| FEV1 (L) | 2.17 | 78% |
| FEV1/FVC (%): | 58 | 80% |
| PEF (L/sec): | 2.97 | 41% |

| Observed: | %Predicted: | |
| FVC (L): | 2.46 | 88% |
| FEV1 (L) | 1.66 | 75% |
| FEV1/FVC (%): | 67 | 83% |
| PEF (L/sec): | 7.65 | 128% |
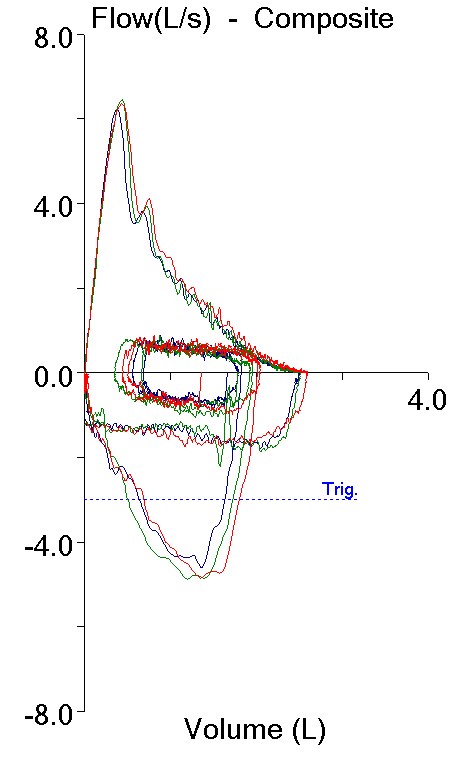
Both tests also showed mild airway obstruction but despite this the Peak Flows were quite different. One test had a PEF that was moderately to severely reduced and the other had a PEF that was elevated. It’s fascinating that two such completely different flow-volume loops are so numerically similar.
In another sense, though, how can these two different spirometry efforts both be labeled as mild airway obstruction? Or more importantly, they both may be mild obstruction but isn’t the quality of the obstruction different?